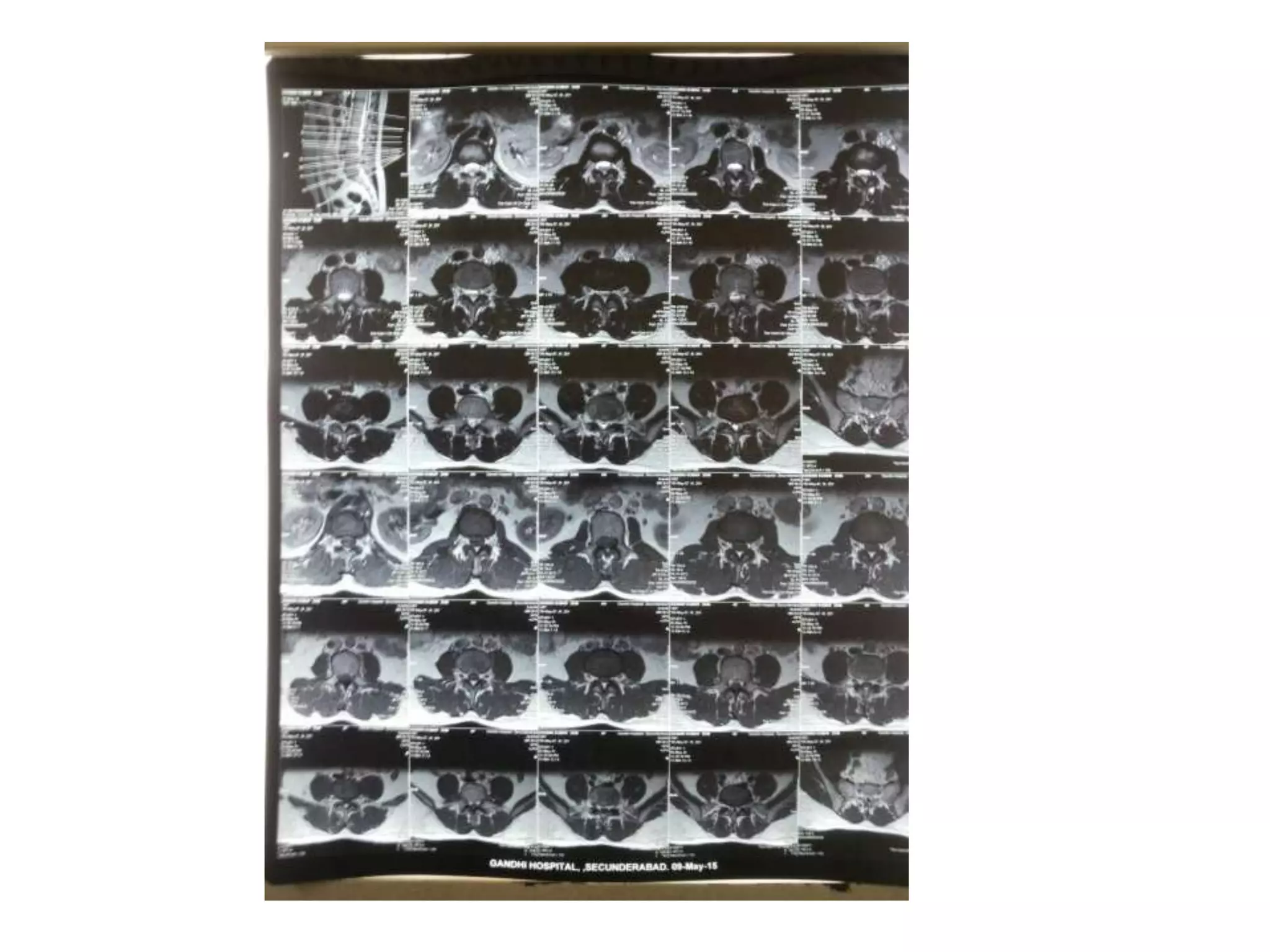
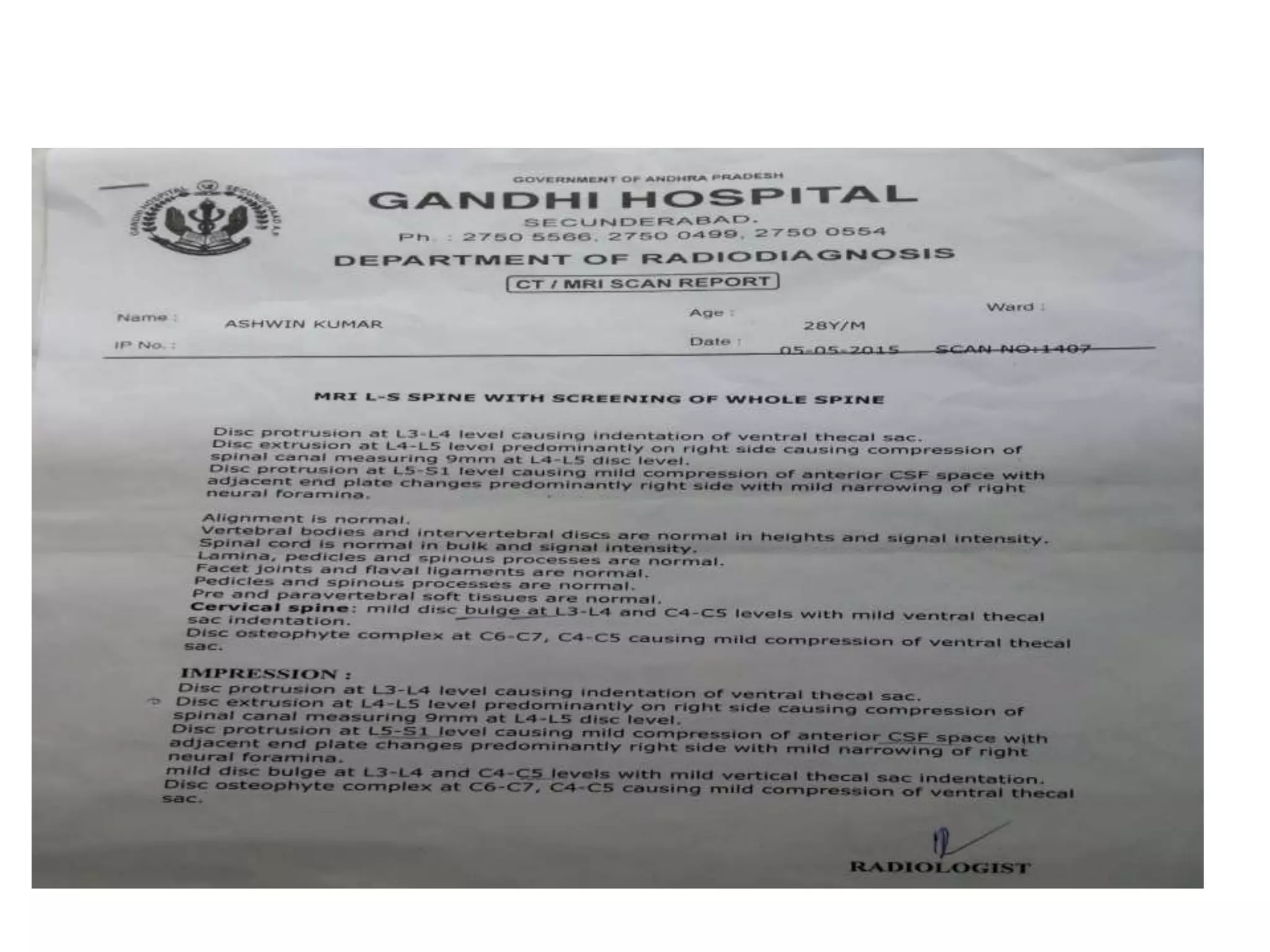
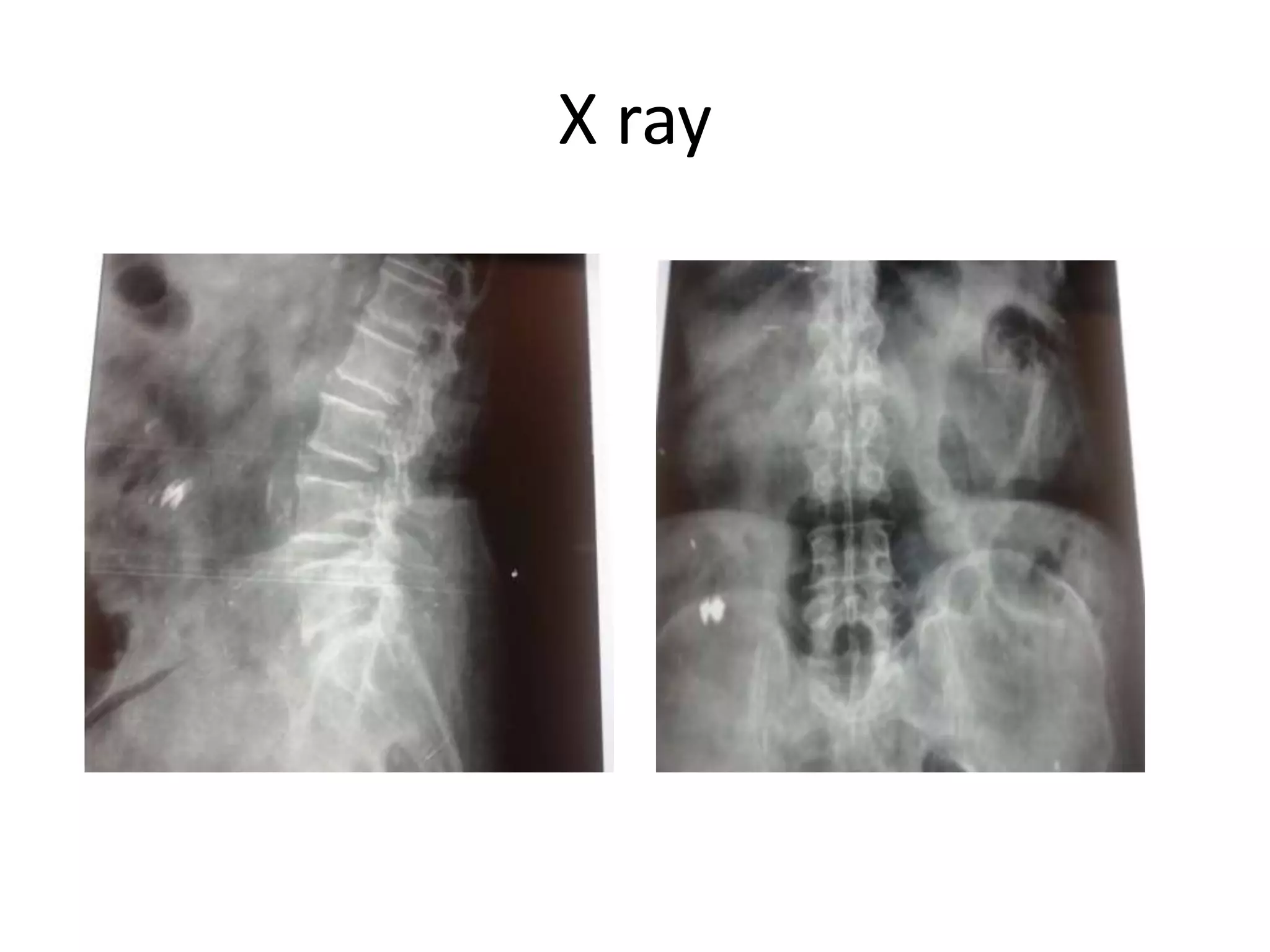
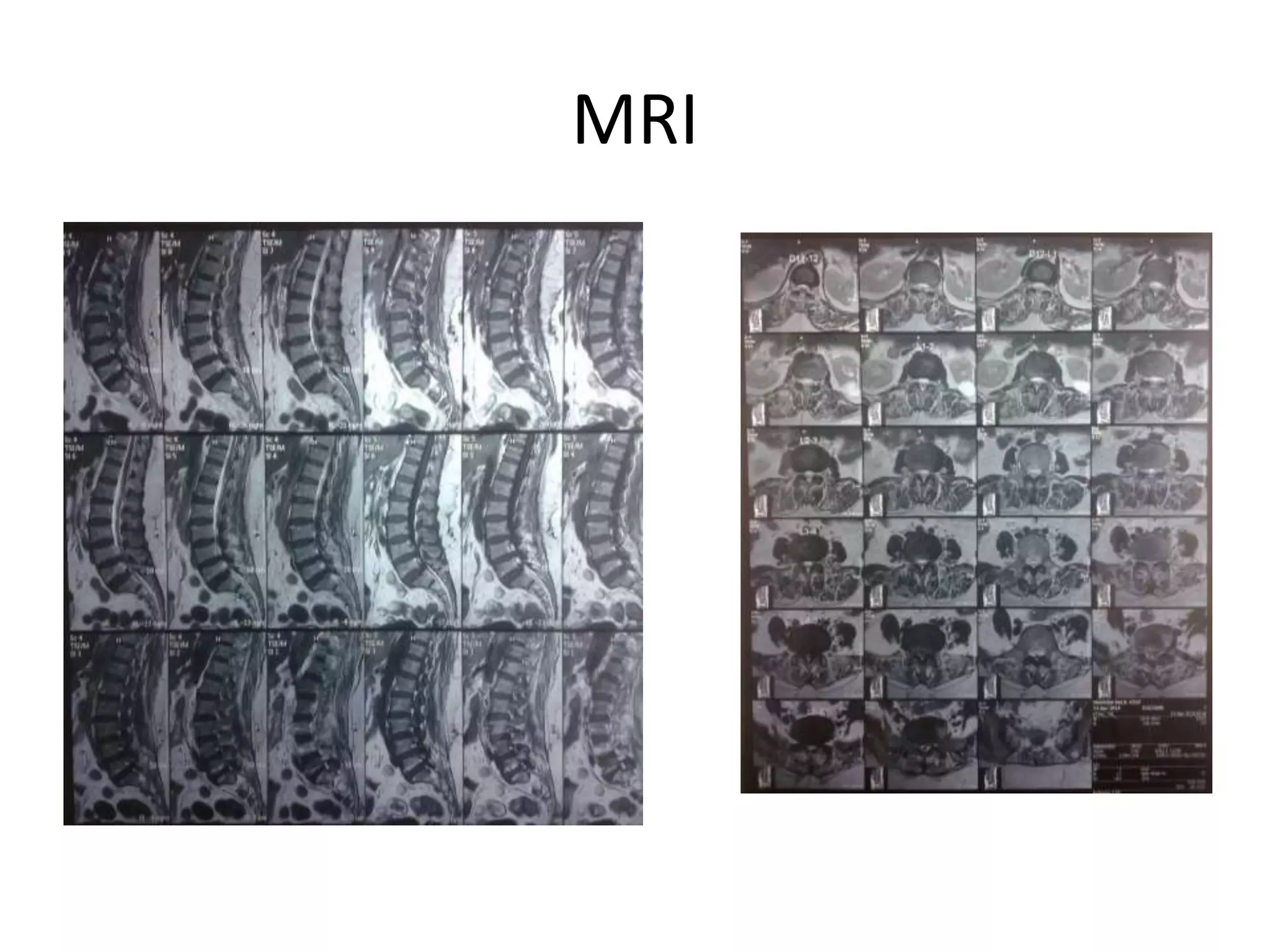
This document presents two clinical case presentations of patients with back pain. The first case involves a 28-year-old male with low back pain radiating to his right leg. Diagnostic tests revealed a prolapsed intervertebral disc at L4-L5 with lumbar canal stenosis. He underwent a laminectomy with discectomy and experienced post-operative relief. The second case involves a 34-year-old male with low back pain radiating to his left leg. Diagnostic tests revealed a prolapsed disc at L4-L5 more pronounced on the left side. He underwent a laminotomy with micro-discectomy at L4-L5 and also experienced post-operative relief.