OUTLINE:
Definition
Anatomy and physiologyof cervix
Incidence of cervical cancer
Etiology & risk factors of cervical cancer
Pathophysiology of cervical cancer
Types of cervical cancer
Clinical manifestations of cervical cancer
Stages of cervical cancer
Diagnostic evaluation of cervical cancer
Medical and Nursing management of cervical cancer
Prevention of cervical cancer
4.
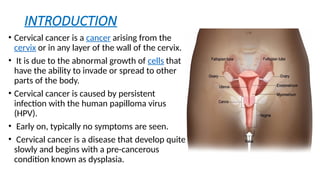
INTRODUCTION
• Cervical canceris a cancer arising from the
cervix or in any layer of the wall of the cervix.
• It is due to the abnormal growth of cells that
have the ability to invade or spread to other
parts of the body.
• Cervical cancer is caused by persistent
infection with the human papilloma virus
(HPV).
• Early on, typically no symptoms are seen.
• Cervical cancer is a disease that develop quite
slowly and begins with a pre-cancerous
condition known as dysplasia.
5.
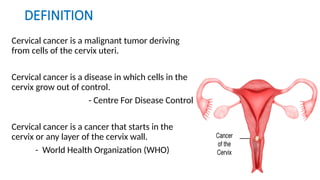
DEFINITION
Cervical cancer isa malignant tumor deriving
from cells of the cervix uteri.
Cervical cancer is a disease in which cells in the
cervix grow out of control.
- Centre For Disease Control
Cervical cancer is a cancer that starts in the
cervix or any layer of the cervix wall.
- World Health Organization (WHO)
6.
INCIDENCE
Globally:
• fourth mostcommon cancer in women with around 660 000 new cases and
around 350 000 deaths in 2022.
In India:
• Third most common cancer in women.
• Around 75000 women die from cervical cancer each year.
• Accounts for 25 % of all global deaths due to cervical cancer.
Tata Memorial Hospital
• Annually, out of 45,000 new cancers seen, approximately 800–1000 new cervix
cancers are diagnosed, of which about 75% undergo complete treatment at TMH.
• The highest rates of cervical cancer incidence and mortality are in low- and
middle-income countries.
• Women living with HIV are 6 times more likely to develop cervical cancer
compared to women without HIV.
7.
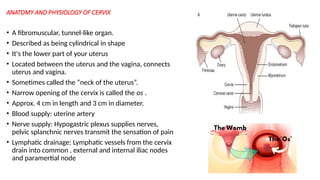
ANATOMY AND PHYSIOLOGYOF CERVIX
• A fibromuscular, tunnel-like organ.
• Described as being cylindrical in shape
• It's the lower part of your uterus
• Located between the uterus and the vagina, connects
uterus and vagina.
• Sometimes called the “neck of the uterus”.
• Narrow opening of the cervix is called the os .
• Approx. 4 cm in length and 3 cm in diameter.
• Blood supply: uterine artery
• Nerve supply: Hypogastric plexus supplies nerves,
pelvic splanchnic nerves transmit the sensation of pain
• Lymphatic drainage: Lymphatic vessels from the cervix
drain into common , external and internal iliac nodes
and paramertial node
8.
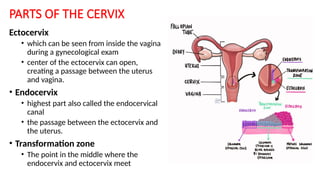
PARTS OF THECERVIX
Ectocervix
• which can be seen from inside the vagina
during a gynecological exam
• center of the ectocervix can open,
creating a passage between the uterus
and vagina.
• Endocervix
• highest part also called the endocervical
canal
• the passage between the ectocervix and
the uterus.
• Transformation zone
• The point in the middle where the
endocervix and ectocervix meet
9.
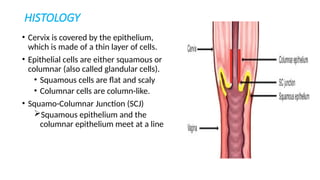
HISTOLOGY
• Cervix iscovered by the epithelium,
which is made of a thin layer of cells.
• Epithelial cells are either squamous or
columnar (also called glandular cells).
• Squamous cells are flat and scaly
• Columnar cells are column-like.
• Squamo-Columnar Junction (SCJ)
Squamous epithelium and the
columnar epithelium meet at a line
10.
FUNCTIONS OF CERVIX
DuringMenstruation
• During menstruation, the cervix opens a small
amount to permit the passage of menstrual blood out
of the uterus and through the vagina.
During Conception
• Conception occurs when sperm travel through the
cervix to enter the uterus and ultimately fertilize an
egg. Around ovulation, the most fertile part of the
menstrual cycle, your cervix produces clear mucus,
which helps the sperm reach the uterus.
11.
During Pregnancy andLabor
• During pregnancy, cervical mucus thickens to create a cervical
"plug" that shields the growing embryo from infection.
• When a pregnant woman gets closer to going into labor,
the cervical plug thins and is expelled. The cervix softens and
shortens (this is called effacement) and then dilates in preparation
for birth.
During Menopause
• During menopause, hormonal changes and aging change the nature
of the cervical mucus and vaginal discharge. As a result, some
menopausal females experience vaginal dryness.
12.
Types of cervicalcancer
• Based on the type of cell in which the cancer begins
• Squamous cell carcinoma
• begins in thin, flat cells, called squamous cells which line the
outer part of the cervix.
• 80% to 90% of cervical cancers
• Adenocarcinoma
• This type of cervical cancer begins in the column-shaped gland
cells that line the cervical canal.
• 10% to 20% are adenocarcinoma
• Can also have a mix of both types.
13.
RISK FACTORS ANDCAUSES
• Some risk factors within your control are:
• Screening history: People who haven’t had Pap tests at regular intervals are more likely to
get cervical cancer (because Pap tests can detect precancerous cells).
• HPV infection: Certain types of HPV cause cervical cancer.
• Sexual history: Having sexual intercourse before the age of 18 and having many sexual
partners may put at higher risk of HPV infection.
• Smoking: Smoking cigarettes increases your risk of cervical cancer.
• HIV infection: People with HIV have a higher-than-average risk of developing cervical cancer.
• Having a weakened immune system: Having a weak immune system makes your body
unable to fight infections.
• Exposure to oral contraceptives & nicotine.
• There are some risk factors you can’t change or control.
• DES (diethylstilbestrol): DES is a medication that was given to people between 1938 and
1971 to prevent miscarriage. If your birth parent took DES, you may be more likely to get
cervical cancer.
• Family history: Cervical cancer may have a genetic component.
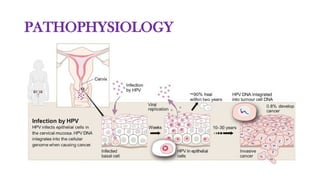
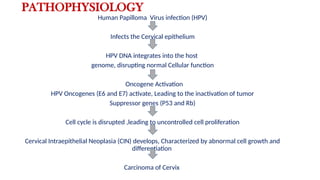
PATHOPHYSIOLOGY
Human Papilloma Virusinfection (HPV)
Infects the Cervical epithelium
HPV DNA integrates into the host
genome, disrupting normal Cellular function
Oncogene Activation
HPV Oncogenes (E6 and E7) activate, Leading to the inactivation of tumor
Suppressor genes (P53 and Rb)
Cell cycle is disrupted ,leading to uncontrolled cell proliferation
Cervical Intraepithelial Neoplasia (CIN) develops, Characterized by abnormal cell growth and
differentiation
Carcinoma of Cervix
16.
CERVICAL CANCER DEVELOPMENT
•Cervical dysplasia is a precancerous condition in which abnormal cells grow on
the surface of your cervix.
• Also called as cervical intraepithelial neoplasia [CIN]
• “Intraepithelial” means that the abnormal cells are present on the surface
(epithelial tissue) of your cervix and have not grown past that surface layer.
• “Neoplasia” refers to the growth of abnormal cells.
• classified on a scale from one to three:
• CIN 1: Refers to abnormal cells affecting about one-third of the thickness of the epithelium.
• CIN 2: Refers to abnormal cells affecting about one-third to two-thirds of the epithelium.
• CIN 3: Refers to abnormal cells affecting more than two-thirds of the epithelium.
CIN 1 cervical dysplasia rarely becomes cancer and often goes away on
its own. CIN 2 and 3 are more likely to require treatment to prevent
cancer.
18.
Vaginal bleeding
that occurs
betweenmenstrual
periods or after
menopause
Leg
swelling
Vaginal discharge
that is thick,
odorous or tinged with
blood
Vaginal bleeding
during a pelvic examination
Vaginal
bleeding or
pain
during sexual
intercourse
Menstrual
periods that are
heavier or last longer than
usual
Painful urination
and
Urinary
urgency or frequency
Pain in the lower
back or pelvic region
CLINICAL
MANIFESTATIONS
19.
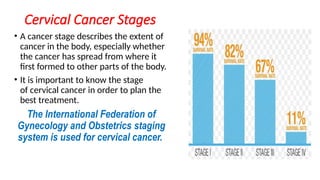
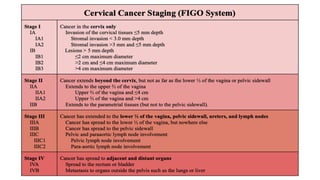
Cervical Cancer Stages
•A cancer stage describes the extent of
cancer in the body, especially whether
the cancer has spread from where it
first formed to other parts of the body.
• It is important to know the stage
of cervical cancer in order to plan the
best treatment.
The International Federation of
Gynecology and Obstetrics staging
system is used for cervical cancer.
20.
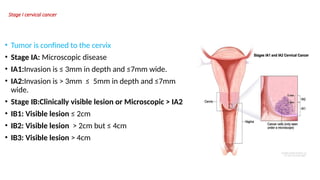
Stage I cervicalcancer
• Tumor is confined to the cervix
• Stage IA: Microscopic disease
• IA1:Invasion is ≤ 3mm in depth and ≤7mm wide.
• IA2:Invasion is > 3mm ≤ 5mm in depth and ≤7mm
wide.
• Stage IB:Clinically visible lesion or Microscopic > IA2
• IB1: Visible lesion ≤ 2cm
• IB2: Visible lesion > 2cm but ≤ 4cm
• IB3: Visible lesion > 4cm
21.
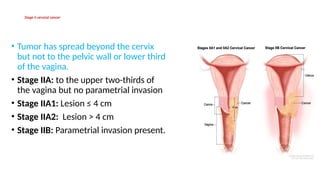
Stage II cervicalcancer
• Tumor has spread beyond the cervix
but not to the pelvic wall or lower third
of the vagina.
• Stage IIA: to the upper two-thirds of
the vagina but no parametrial invasion
• Stage IIA1: Lesion ≤ 4 cm
• Stage IIA2: Lesion > 4 cm
• Stage IIB: Parametrial invasion present.
22.
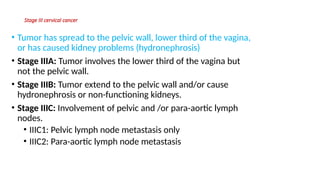
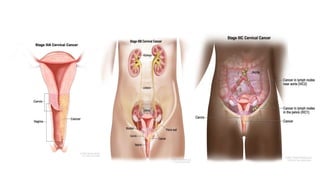
Stage III cervicalcancer
• Tumor has spread to the pelvic wall, lower third of the vagina,
or has caused kidney problems (hydronephrosis)
• Stage IIIA: Tumor involves the lower third of the vagina but
not the pelvic wall.
• Stage IIIB: Tumor extend to the pelvic wall and/or cause
hydronephrosis or non-functioning kidneys.
• Stage IIIC: Involvement of pelvic and /or para-aortic lymph
nodes.
• IIIC1: Pelvic lymph node metastasis only
• IIIC2: Para-aortic lymph node metastasis
24.
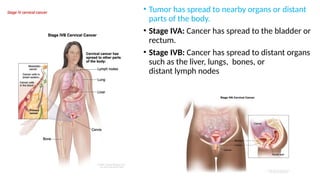
Stage IV cervicalcancer • Tumor has spread to nearby organs or distant
parts of the body.
• Stage IVA: Cancer has spread to the bladder or
rectum.
• Stage IVB: Cancer has spread to distant organs
such as the liver, lungs, bones, or
distant lymph nodes
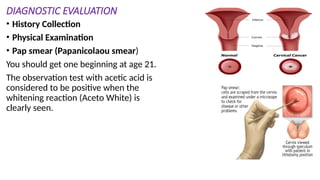
DIAGNOSTIC EVALUATION
• HistoryCollection
• Physical Examination
• Pap smear (Papanicolaou smear)
You should get one beginning at age 21.
The observation test with acetic acid is
considered to be positive when the
whitening reaction (Aceto White) is
clearly seen.
28.
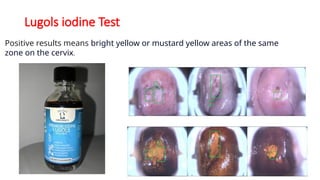
Lugols iodine Test
Positiveresults means bright yellow or mustard yellow areas of the same
zone on the cervix.
29.
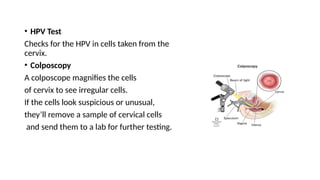
• HPV Test
Checksfor the HPV in cells taken from the
cervix.
• Colposcopy
A colposcope magnifies the cells
of cervix to see irregular cells.
If the cells look suspicious or unusual,
they’ll remove a sample of cervical cells
and send them to a lab for further testing.
30.
Methods to geta sample of tissue from your cervix:
• Punch biopsy:
uses a cutting tool with a round top to cut out the precancerous cells.
• Endocervical curettage:
A procedure that involves scraping the lining of cervix with a spoon-shaped tool called a
curette.
• Loop electrosurgical excision procedure (LEEP):
uses an electrical wire loop to remove the abnormal cervical tissue.
• Cone biopsy:
removes a slightly larger, cone-shaped piece of tissue from cervix.
• Cystoscopy
uses a thin, tube-like instrument with a light and a lens for viewing inside
• Proctoscopy
Uses a short, straight, rigid, hollow metal tube, and usually has a small light bulb at end
31.
If the resultsfrom these test confirms cervical cancer, further tests will
determine whether the disease has spread (metastasized). These tests
might include:
• Liver and kidney function studies
• Blood and urine tests
• X-rays
• CT scans
• PET-CT scans
• MRI
• Intravenous Urography /Intravenous Pyelogram
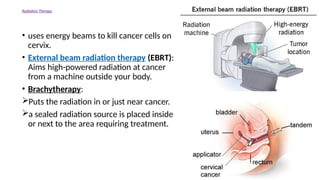
Radiation Therapy
• usesenergy beams to kill cancer cells on
cervix.
• External beam radiation therapy (EBRT):
Aims high-powered radiation at cancer
from a machine outside your body.
• Brachytherapy:
Puts the radiation in or just near cancer.
a sealed radiation source is placed inside
or next to the area requiring treatment.
34.
Chemotherapy
• Chemotherapy usesdrugs injected
into your veins or taken by mouth to
kill cancer cells.
For Example:
cisplatin, carboplatin, ifosfamide ,
irinotecan, gemcitabine, paclitaxel,
topotecan and vinorelbine .
These drugs may be given alone or in
combination.
35.
Targeted therapy
• Drugdestroys specific cancer
cells without damaging healthy
cells.
• It works by targeting proteins
that control how cancer cells
grow and spread.
For Example:
• Bevacizumab (Avastin, Bevatas,
Bryxta)
• Trastuzumab (Eleftha , Vivitra )
36.
Immunotherapy
• Immunotherapy usesmedicine to
stimulate your immune system to
recognize and destroy cancer cells.
• Cancer cells pretend to be healthy to
hide from your immune system.
• Immunotherapy helps target these
signals so the cancer cells can’t trick
your body into thinking it’s a healthy
cell.
For Example:
• Pembrolizumab (Keytruda)
37.
Hormone therapy blocksthe production or the
effects of the hormones and helps stop the
cancer from growing.
38.
to treat pre-cancersof the
cervix:
• Ablation destroys cervical
tissue with cold
temperatures
(cryosurgery) or with
a laser (laser ablation)
rather than removing it.
• Excisional surgery
(conization) cuts out and
removes the pre-cancer.
SURGICAL
MANAGEMENT
39.
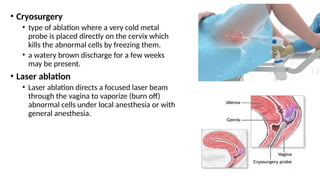
• Cryosurgery
• typeof ablation where a very cold metal
probe is placed directly on the cervix which
kills the abnormal cells by freezing them.
• a watery brown discharge for a few weeks
may be present.
• Laser ablation
• Laser ablation directs a focused laser beam
through the vagina to vaporize (burn off)
abnormal cells under local anesthesia or with
general anesthesia.
40.
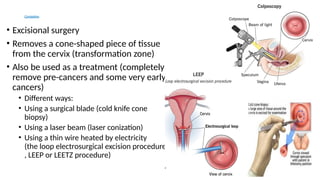
Conization
• Excisional surgery
•Removes a cone-shaped piece of tissue
from the cervix (transformation zone)
• Also be used as a treatment (completely
remove pre-cancers and some very early
cancers)
• Different ways:
• Using a surgical blade (cold knife cone
biopsy)
• Using a laser beam (laser conization)
• Using a thin wire heated by electricity
(the loop electrosurgical excision procedure
, LEEP or LEETZ procedure)
41.
Surgery for invasivecervical cancer
Hysterectomy (simple or radical) Trachelectomy
42.
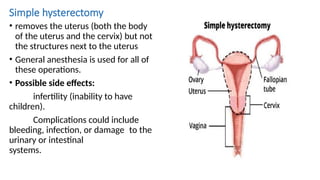
Simple hysterectomy
• removesthe uterus (both the body
of the uterus and the cervix) but not
the structures next to the uterus
• General anesthesia is used for all of
these operations.
• Possible side effects:
infertility (inability to have
children).
Complications could include
bleeding, infection, or damage to the
urinary or intestinal
systems.
43.
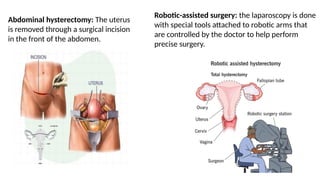
Abdominal hysterectomy: Theuterus
is removed through a surgical incision
in the front of the abdomen.
Robotic-assisted surgery: the laparoscopy is done
with special tools attached to robotic arms that
are controlled by the doctor to help perform
precise surgery.
44.
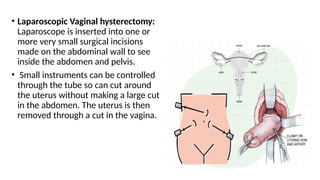
• Laparoscopic Vaginalhysterectomy:
Laparoscope is inserted into one or
more very small surgical incisions
made on the abdominal wall to see
inside the abdomen and pelvis.
• Small instruments can be controlled
through the tube so can cut around
the uterus without making a large cut
in the abdomen. The uterus is then
removed through a cut in the vagina.
45.
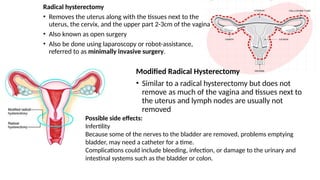
Radical hysterectomy
• Removesthe uterus along with the tissues next to the
uterus, the cervix, and the upper part 2-3cm of the vagina
• Also known as open surgery
• Also be done using laparoscopy or robot-assistance,
referred to as minimally invasive surgery.
Modified Radical Hysterectomy
• Similar to a radical hysterectomy but does not
remove as much of the vagina and tissues next to
the uterus and lymph nodes are usually not
removed
Possible side effects:
Infertility
Because some of the nerves to the bladder are removed, problems emptying
bladder, may need a catheter for a time.
Complications could include bleeding, infection, or damage to the urinary and
intestinal systems such as the bladder or colon.
46.
Trachelectomy
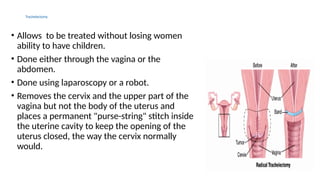
• Allows tobe treated without losing women
ability to have children.
• Done either through the vagina or the
abdomen.
• Done using laparoscopy or a robot.
• Removes the cervix and the upper part of the
vagina but not the body of the uterus and
places a permanent "purse-string" stitch inside
the uterine cavity to keep the opening of the
uterus closed, the way the cervix normally
would.
47.
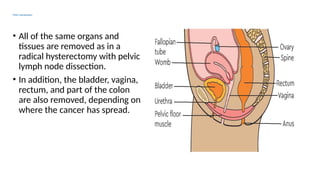
Pelvic Exenteration
• Allof the same organs and
tissues are removed as in a
radical hysterectomy with pelvic
lymph node dissection.
• In addition, the bladder, vagina,
rectum, and part of the colon
are also removed, depending on
where the cancer has spread.
48.
Nursing Management
• Assessment
•Gynecological Assessment:
• Monitor for vaginal bleeding, discharge, and any signs of infection.
• Pain Assessment:
• Evaluate the location, intensity, and nature of pelvic pain.
• Nutritional Status Assessment:
• Monitor for signs of weight loss or malnutrition.
• Psychosocial Assessment:
• Assess emotional and psychological responses to the diagnosis and treatment.
49.
Nursing Diagnosis
1. AcutePain related to tumor growth and treatment effects as
evidenced by pain scale / facial expression.
2. Anxiety related to cancer diagnosis and treatment uncertainties as
evidenced by talking with family members.
3. Risk for Infection related to immune suppression.
4. Impaired urinary elimination related to surgical incision.
5. Altered nutrition less than body requirements related to anorexia /
vomiting as evidenced by weight loss.
50.
Acute Pain relatedto tumor growth and treatment effects as
evidenced by pain scale / facial expression.
• 1. Encourage the patient to use non-pharmacologic pain relief interventions.
Massage, meditation, heat, and other diversional activities promote relaxation and pain relief.
• 2. Administer pain relief medications as needed.
Opioids and NSAIDs may be prescribed to help manage pain in patients with cancer.
Acetaminophen and weak opioids like Tramdol in mild to moderate pain
Morphine as the first option in cases of moderate to severe pain
• 3. Educate the patient about the pain management plan.
Improved control of pain is achieved when the patient has a better understanding of the nature
of the pain, its causes, and treatment.
• 4. Offer resources for coping with the psychological impacts of pain.
Cancer pain affects all aspects of the patient’s well-being. Cognitive behavioral strategies can
help the patient with coping with discomfort and other unpleasant effects of pain.
• 5. Encourage complementary therapies if not contraindicated.
Complementary therapies like acupuncture, yoga, aromatherapy, and hypnotherapy can help
relieve pain without the adverse effects of medication.
51.
Anxiety related tocancer diagnosis and treatment uncertainties as evidenced by talking with family
members.
• Encourage the patient to verbalize thoughts and feelings.
Acknowledging the patient’s feelings and emotions about the cancer diagnosis and
imminent death enhances trust and a therapeutic relationship.
• 2. Educate the patient about the stages of grief.
Understanding the grieving process will reinforce the normality of feelings
experienced by the patient after a cancer diagnosis, allowing them to deal with
grieving more efficiently.
• 3. Encourage family members to be involved in patient care.
A reliable support system will help the patient feel less isolated. Encourage the
patient to lean on their friends and family for support.
• 4. Refer to grief counseling.
Counselors and spiritual advisors can assist the patient with their feelings of anxiety
and anticipatory grieving.
52.
Risk for Infectionrelated to immune suppression.
• 1. Encourage infection control measures.
Frequent hand washing protects the patient from infection. Screening visitors and placing
the patient in isolation will help reduce the risk of airborne and droplet infections.
• 2. Remain home when possible.
Patients with cancer should reduce their interaction with lots of people such as in stores or
restaurants. When venturing out, a mask should be worn to reduce the transmission of
diseases.
• 3. Provide adequate rest periods but remain active.
Ensuring that the patient has adequate rest periods reduces the incidence of fatigue while
adequate exercise can prevent the loss of muscle function and support healthy immune
function.
• 4. Alert the healthcare team to signs of infection.
Ensure the patient knows to alert the healthcare team to any symptoms such as a fever,
cough, chills, sore throat, or mouth sores.
• 5. Maintain asepsis of invasive lines.
Maintain sterile technique when changing a PICC dressing or accessing a port to prevent
introducing bacteria. Clean urinary catheters daily and discontinue once appropriate.
53.
Impaired urinary eliminationrelated to surgical incision.
• Educate on bladder training. Patients with incontinence or an
overactive bladder can teach their bladders to increase the amount of
urine to hold.
• Encourage water intake.Proper hydration promotes
urinary .elimination by maintaining renal function and flushing
bacteria and waste products.
• Limit other fluids.Patients should limit their intake of coffee and
caffeine, carbonated beverages, and alcohol as these can be irritating
to the bladder and cause increased frequency and urgency
• Educate on medications. If ordered by a physician, medications can
help with retention and overactive bladder.
54.
Altered nutrition lessthan body requirements related to
anorexia / vomiting as evidenced by weight loss.
• Complete a thorough nutrition assessment.
• Assess the reason for imbalanced nutrition
• Assess oral care/hygiene.
• Provide good oral hygiene.
Good oral hygiene can increase an individual’s appetite.
• Educate the patient on the body’s nutritional needs.
This will allow the patient to gain knowledge in the area of how to
independently care for oneself
• Administer antiemetics as needed before meals.
Providing appropriate antiemetics will allow for the patient’s appetite to
potentially increase and tolerate intake better.
55.
COMPLICATIONS
• Early menopause
•Narrowing of the vagina
• Lymphoedema
• Emotional impact(Depression)
• Pain
• Kidney failure
• Blood clots
• Bleeding
• Fistula
• Vaginal discharge
56.
PREVENTION
• Human papillomavirus(HPV) vaccine
• Gardasil 9
• Cervarix : It is used to prevent the disease caused by HPV types 16 and 18.
• Screening tests
• Two screening tests can help find changes that could become precancer or
cervical cancer:
• The Pap test (or Pap smear) looks for precancers, cell changes on the cervix
that might become cervical cancer if they are not treated appropriately.
• The HPV test looks for the virus (human papillomavirus) that can cause these
cell changes. These things may also help lower your risk for cervical cancer:
• Don't smoke.
• Use condoms during sex.
57.
CERVARIX
CERVARIX (available since2009)
Human papillomavirus vaccine [types 16, 18]
DOSAGE AND ADMINISTRATION
Two or three doses (0.5-mL each) by intramuscular injection according
to the following schedule:
Patients 9 through 14 years
Regimen Schedule
2-dose 0, 5 to 13 months
3-dose 0, 2, 6 months
58.
GARDASIL 9 (availablesince 2014)
GARDASIL 9 prevents from human papillomavirus (HPV) Types 16, 18,
31, 33, 45, 52, 58 6 and 11.
GARDASIL 9 should be administered
intramuscularly in the deltoid or
anterolateral area of the thigh.
BIBLIOGRAPHY
• Devita VT,Lawrence TS,Rosenberg SA, Cancer : Principle & Practice of oncology. 11th
ed.
Philadelphia, PA Woltres Kluwer ; 2019
• Smeltzer SC, Bare BG. Brunner and Suddarths Textbook of Medical- Surgical Nursing, 14th
ed.
Philadelphia ,PA : Wolters Kluwer : 2022
• Ignatavicius DD, Workman ML .Medical- Surgical Nursing :Patient Centered Collaborative
Care. 9th
ed. St Louis MO : Elsevier : 2020
• American Cancer Society. (2022).Cervical Cancer. Available From http://www.cancer.org
• World Health Organization .(2024) Cervical Cancer Available From
https://www.who.int/health-topics/cervical-cancer#tab=tab-1
• https:www.mayoclinic.org/diseases-conditions/cervical-cancer/symptoms-causes/Syc-
20352501.
• National Cancer Institute .Cervical Cancer .Available From
http:www.cancer.gov/types/cervical


![CERVICAL CANCER DEVELOPMENT
• Cervical dysplasia is a precancerous condition in which abnormal cells grow on
the surface of your cervix.
• Also called as cervical intraepithelial neoplasia [CIN]
• “Intraepithelial” means that the abnormal cells are present on the surface
(epithelial tissue) of your cervix and have not grown past that surface layer.
• “Neoplasia” refers to the growth of abnormal cells.
• classified on a scale from one to three:
• CIN 1: Refers to abnormal cells affecting about one-third of the thickness of the epithelium.
• CIN 2: Refers to abnormal cells affecting about one-third to two-thirds of the epithelium.
• CIN 3: Refers to abnormal cells affecting more than two-thirds of the epithelium.
CIN 1 cervical dysplasia rarely becomes cancer and often goes away on
its own. CIN 2 and 3 are more likely to require treatment to prevent
cancer.](https://image.slidesharecdn.com/cacervix-250427074012-f0043d7d/85/Ca-Cervix-pptx-ca-cervix-ca-cervix-ca-cervix-16-320.jpg)



![CERVARIX
CERVARIX (available since 2009)
Human papillomavirus vaccine [types 16, 18]
DOSAGE AND ADMINISTRATION
Two or three doses (0.5-mL each) by intramuscular injection according
to the following schedule:
Patients 9 through 14 years
Regimen Schedule
2-dose 0, 5 to 13 months
3-dose 0, 2, 6 months](https://image.slidesharecdn.com/cacervix-250427074012-f0043d7d/85/Ca-Cervix-pptx-ca-cervix-ca-cervix-ca-cervix-57-320.jpg)