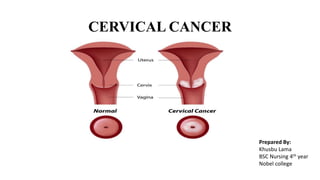
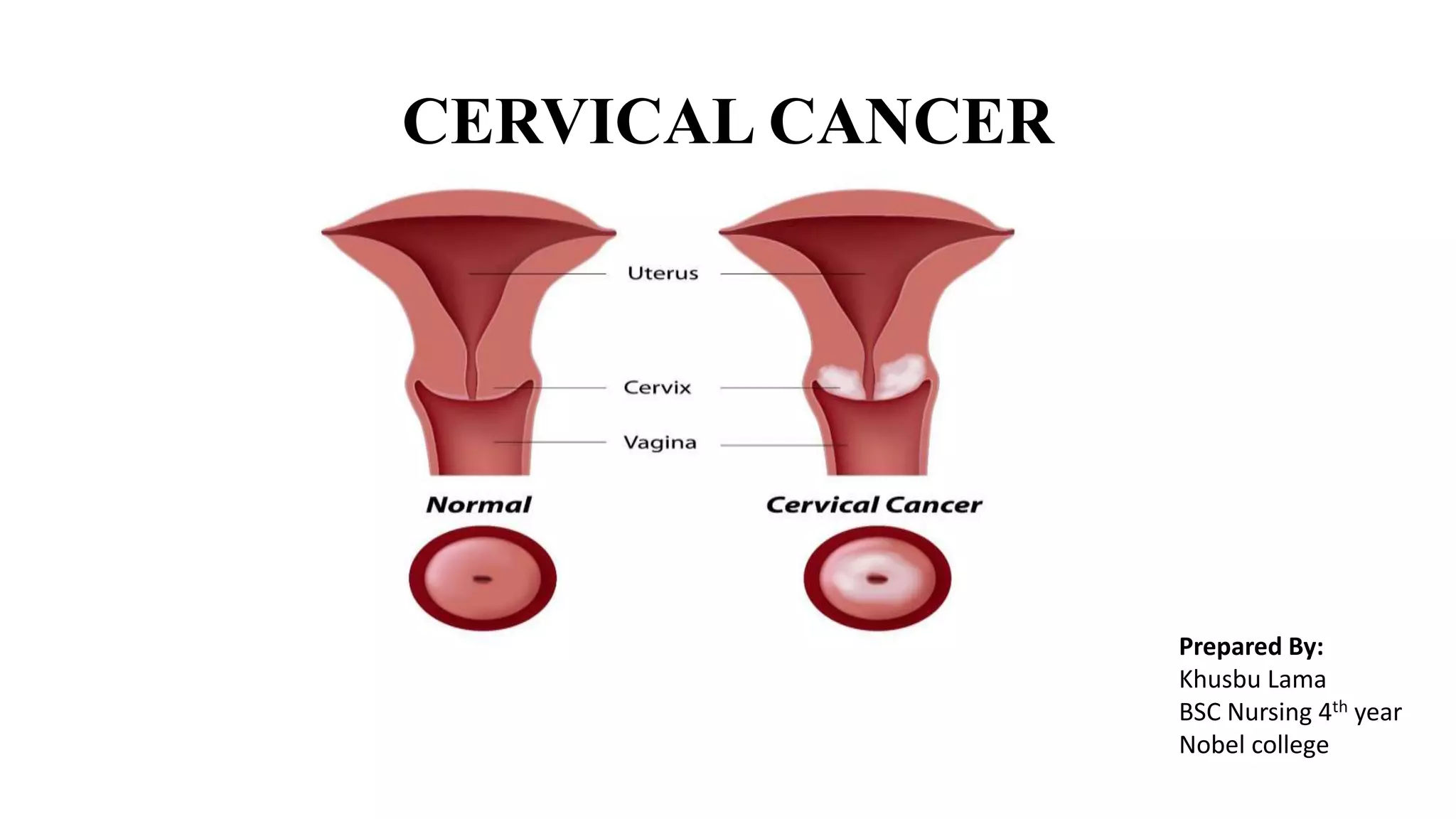
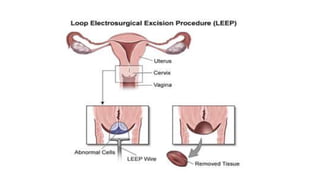
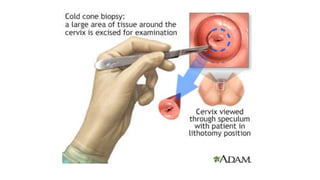
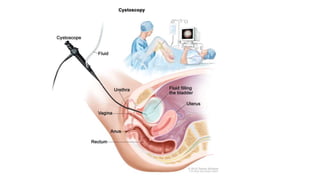
Cervical cancer is caused by HPV infection and develops in the lining of the cervix. It ranges from early stage cancers contained within the cervix to late stages that spread beyond the cervix. Symptoms can include abnormal bleeding or discharge. Diagnosis involves tests like Pap smears, biopsies, and imaging. Treatment options depend on the stage and include surgery, radiation, chemotherapy, or a combination. Regular screening and HPV vaccination can help prevent cervical cancer.