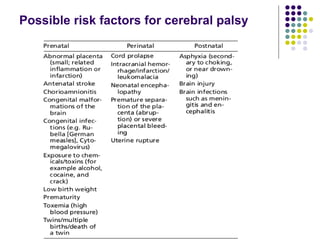

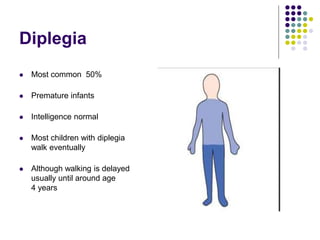
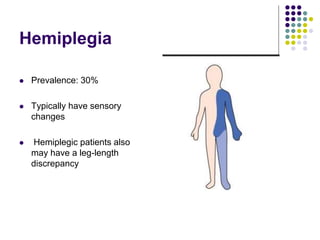
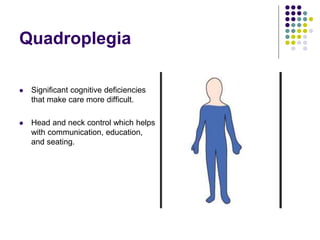
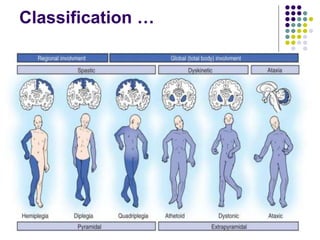
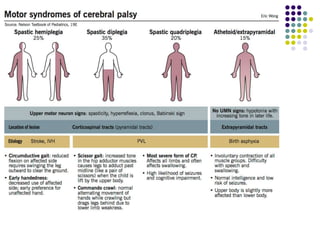

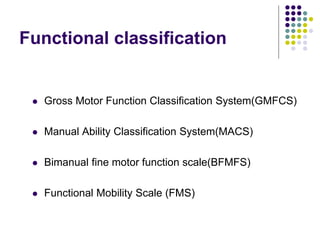
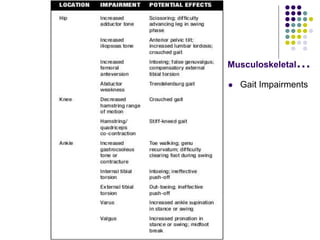



The document provides information on cerebral palsy, including: - It was first described in 1862 and the term originated with Freud. - It is a non-progressive disorder of motor development caused by disturbances in the developing brain. - Symptoms can include developmental delays, abnormal muscle tone and movement patterns, unusual posture, and early hand preference. - It is classified based on affected limbs (diplegia, hemiplegia, quadriplegia) and physiological characteristics (spastic, dyskinetic, ataxic, hypotonic). - Assessments evaluate multiple body systems and functions like posture, mobility, sensation, and fine motor skills.




























































![cerebral palsy[1].pptxcerebral palsy management etiopathogenesis](https://cdn.slidesharecdn.com/ss_thumbnails/cerebralpalsy1-251219125140-a80c6a48-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












