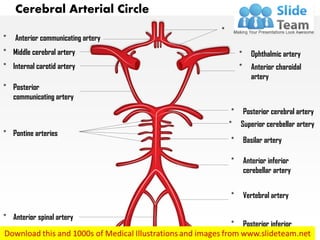
This document contains diagrams of the cerebral arterial circle with labels. It includes diagrams with labels removed and a highlighted section. The text provides instructions on how to edit the diagrams in PowerPoint by adding text boxes, changing colors, sizes, and adding custom labels and highlights. The goal is to bring presentations to life by editing and customizing the diagrams.
Atlanto occipital and atlanto axial jointShubham Singh
Anatomy:
>Atlas is the topmost vertebra and chief peculiarity of atlas is that it has no body, it is ring like and consist of anterior and posterior arch and two lateral masses.
>Axis, the 2nd cervical vertebra has a concave under side and convex from side to side. The most distinctive characteristic of this bone is strong odontoid process, the dens.
TheJoint:
>Atlanto-occipital joint (articulation between the atlas and the occipital bone) consists of a pair of condyloid joints.
>The atlanto-occipital joints are synovial socket-type joints
Ligaments:
> Posterior atlanto-occipital membrane: extend from anterior arch of atlas to posterior margin of foramen magnum.
>Anterior atlanto-occipital membrane: extend from anterior arch of atlas to anterior margin of foramen magnum.
>The ligamentam flavam join laminae of adjacent vertebral arches.
>The interspinous ligaments expand to form the ligamentum nuchae which inserts along the posterior foramen magnum and external occipital condyle.
> The following four ligaments stabilize these joints:
1.Apical ligament: Connects the dens to the foramen magnum of the occipital bone.
2.Alar ligaments: Connect the dens to the lateral margins of the foramen magnum.
3.Cruciate ligament: Attaches the dens to the anterior arch of the atlas and the body of the axis to the foramen magnum of the occipital bone.
4.Tectorial membrane: Starts at the skull and becomes the posterior longitudinal ligament.
>Atlanto-axial articular capsules are thick and loose, and connect the margins of the lateral masses of the atlas with those of the posterior articular surfaces of the axis.
Muscles:
>Flexion is produced mainly by the action of longis capitis, rectus capitis anterior and sternocleidomastoid (anterior fibres)
>Extension by the rectus capitis posterior major and minor, the obliquus capitis superior, the semispinalis capitis, splenius capitis, longissimus capitis, sternocleidomastoid and upper fibres of the trapezius
>The recti lateralis are concerned in the lateral movement, assisted by the trapezius, splenius capitis, semispinalis capitis, and the sternocleidomastoid of the same side, all acting together.
Movements:
>Flexion and extension in the Sagittal axis, which give rise to the ordinary forward and backward nodding of the head.
>Lateral flexion to one or other side in the Frontal axis(titling of head
>Lateral AAJ Movement: It is a synovial joint which allows only gliding
>Medial AAJ Movement: This joint allows the rotation of the atlas the axis i.e round the dens.
Clinical anatomy:
> Headaches can arise from many different sources including dysfunctional muscles, tears in the ligaments, misalignment of the vertebral bodies, injury to cervical facets and degenerative discs.
>Excessive flexion could rupture the supraspinous ligament.
>Posterior atlanto-occipital membrane ossification cause migraine headaches due to compression of artery.
Atlanto occipital and atlanto axial jointShubham Singh
Anatomy:
>Atlas is the topmost vertebra and chief peculiarity of atlas is that it has no body, it is ring like and consist of anterior and posterior arch and two lateral masses.
>Axis, the 2nd cervical vertebra has a concave under side and convex from side to side. The most distinctive characteristic of this bone is strong odontoid process, the dens.
TheJoint:
>Atlanto-occipital joint (articulation between the atlas and the occipital bone) consists of a pair of condyloid joints.
>The atlanto-occipital joints are synovial socket-type joints
Ligaments:
> Posterior atlanto-occipital membrane: extend from anterior arch of atlas to posterior margin of foramen magnum.
>Anterior atlanto-occipital membrane: extend from anterior arch of atlas to anterior margin of foramen magnum.
>The ligamentam flavam join laminae of adjacent vertebral arches.
>The interspinous ligaments expand to form the ligamentum nuchae which inserts along the posterior foramen magnum and external occipital condyle.
> The following four ligaments stabilize these joints:
1.Apical ligament: Connects the dens to the foramen magnum of the occipital bone.
2.Alar ligaments: Connect the dens to the lateral margins of the foramen magnum.
3.Cruciate ligament: Attaches the dens to the anterior arch of the atlas and the body of the axis to the foramen magnum of the occipital bone.
4.Tectorial membrane: Starts at the skull and becomes the posterior longitudinal ligament.
>Atlanto-axial articular capsules are thick and loose, and connect the margins of the lateral masses of the atlas with those of the posterior articular surfaces of the axis.
Muscles:
>Flexion is produced mainly by the action of longis capitis, rectus capitis anterior and sternocleidomastoid (anterior fibres)
>Extension by the rectus capitis posterior major and minor, the obliquus capitis superior, the semispinalis capitis, splenius capitis, longissimus capitis, sternocleidomastoid and upper fibres of the trapezius
>The recti lateralis are concerned in the lateral movement, assisted by the trapezius, splenius capitis, semispinalis capitis, and the sternocleidomastoid of the same side, all acting together.
Movements:
>Flexion and extension in the Sagittal axis, which give rise to the ordinary forward and backward nodding of the head.
>Lateral flexion to one or other side in the Frontal axis(titling of head
>Lateral AAJ Movement: It is a synovial joint which allows only gliding
>Medial AAJ Movement: This joint allows the rotation of the atlas the axis i.e round the dens.
Clinical anatomy:
> Headaches can arise from many different sources including dysfunctional muscles, tears in the ligaments, misalignment of the vertebral bodies, injury to cervical facets and degenerative discs.
>Excessive flexion could rupture the supraspinous ligament.
>Posterior atlanto-occipital membrane ossification cause migraine headaches due to compression of artery.
Making PrescriptionsPpersonal - Pharmacogenomics reports - Software in MedicineGDG Budapest
10 éven belül valóra válhatna az a még
kissé futurisztikusnak tűnő kép, hogy mindenkiről egy genetikai
polimorfizmus adattár áll rendelkezésre mondjuk a háziorvosnál
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
3. Middle cerebral artery
• Download this awesome
diagram. Bring your
presentation to life.
• Bring your presentation to
life.
• Capture your audience’s
attention.
• All image are 100% editable
in power point.
• Download this awesome
diagram.
• Pitch your ideas convincingly.
• Download this awesome
diagram.
Cerebral Arterial Circle – With Highlighted Part
4. Internal carotid artery
• Download this awesome
diagram. Bring your
presentation to life.
• Bring your presentation to
life.
• Capture your audience’s
attention.
• All image are 100% editable
in power point.
• Download this awesome
diagram.
• Pitch your ideas convincingly.
• Download this awesome
diagram.
Cerebral Arterial Circle – With Highlighted Part
5. Anterior inferior cerebellar artery
• Download this awesome
diagram. Bring your
presentation to life.
• Bring your presentation to
life.
• Capture your audience’s
attention.
• All image are 100% editable
in power point.
• Download this awesome
diagram.
• Pitch your ideas convincingly.
• Download this awesome
diagram.
Cerebral Arterial Circle – With Highlighted Part
6. Posterior inferior cerebellar artery
• Download this awesome
diagram. Bring your
presentation to life.
• Bring your presentation to
life.
• Capture your audience’s
attention.
• All image are 100% editable
in power point.
• Download this awesome
diagram.
• Pitch your ideas convincingly.
• Download this awesome
diagram.
Cerebral Arterial Circle – With Highlighted Part
7. " Add your Own Labels and Highlight Any section"
Middle cerebral artery
9. Add Text
1) Open the PowerPoint Slide in which you have to insert the Text Box. Then click on the “Insert
Tab’ in the Ribbon and then inside the Insert Tab, in the ‘Text’ category click on the “Text Box”
icon.
2) Now to insert the Text box, click on the Portion of the Slide where you want the Text box to be
inserted. Once you click, the Text box will be inserted. You can change the size and the shape of
the Text box as per your requirements.
3) Now click on the Text box to enter data into it.
1 2
3
10. 1. Select the shape to change the color and Right click the object( click any object which you
want to change color)
2. Choose Format Shape in the dialog box.
3. Choose “Fill” in the Format Shape box then “Solid” or “Gradient” depending on the
appearance of the object. Change colour as shown in the picture.
Change Color
1
2 3
11. 1. Select the shape to change the size.
2. Click the mouse in the corner of the shape and drag the mouse.
Change Size
1
2