Downloaded 33 times

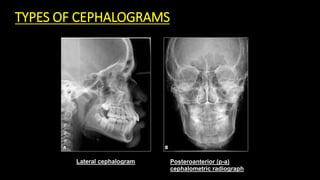
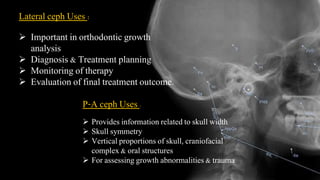
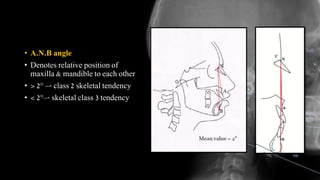


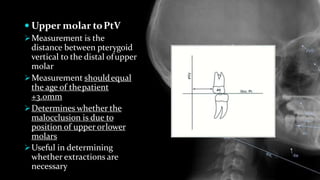
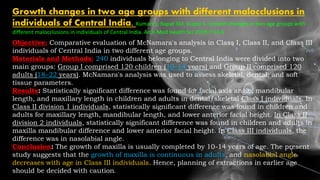



This document provides an overview of cephalometrics and cephalometric analysis. It discusses the history and development of cephalometrics, types of cephalograms, cephalometric landmarks, planes, errors, and classifications of cephalometric analysis including Hard Tissue Analysis methods like Downs analysis and Steiner analysis. Downs analysis uses 10 parameters to evaluate skeletal and dental relationships while Steiner analysis divides analysis into skeletal, dental and soft tissue components to provide maximal information. Cephalometrics is important for orthodontic diagnosis and treatment planning.













































![ceph_LLP_SEMINAR[2].pptx landmarks lines and planes](https://cdn.slidesharecdn.com/ss_thumbnails/cephllpseminar2-250919182304-905904ac-thumbnail.jpg?width=640&height=640&fit=bounds)