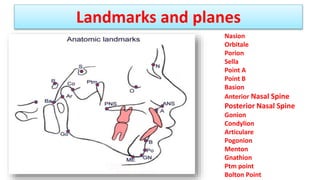
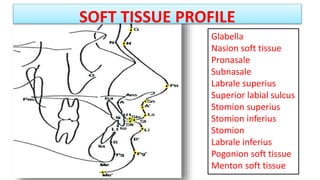
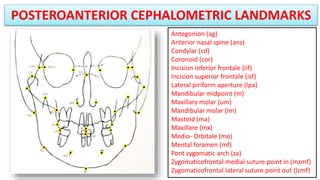
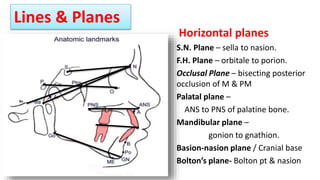
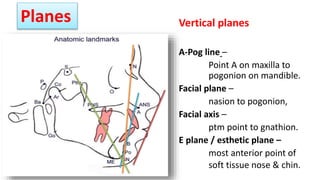
This document discusses the role of cephalometrics in orthodontics, detailing its history, methodologies, and applications in diagnosing cranio-facial structures. It defines cephalometric analysis, outlines types of cephalograms, and elaborates on their uses, including assessment for surgery and orthodontic treatment planning. Additionally, technical aspects of cephalometric radiographs, landmark identification, evaluation methods, and examples of landmarks are described.