Understanding 1st & 2nd Generation Cephalosporins
•Download as DOC, PDF•
4 likes•1,701 views

Cephalosporins are a class of beta-lactam antibiotics derived from the fungus Cephalosporium. They are grouped into generations based on their spectrum of antibacterial activity and resistance to beta-lactamases. First generation cephalosporins are effective against gram-positive organisms but have limited activity against gram-negatives. Second generation have greater activity against gram-negatives like Haemophilus influenzae but less against gram-positives. Third generation have even broader gram-negative coverage and better central nervous system penetration. Clinical uses include surgical prophylaxis, treatment of streptococcal and staphylococcal infections, and therapy for infections caused by Haemophilus, Klebsiella

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Understanding 1st & 2nd Generation Cephalosporins
Similar to Understanding 1st & 2nd Generation Cephalosporins (20)
More from National Academy of Young Scientists
More from National Academy of Young Scientists (17)
Recently uploaded
Recently uploaded (20)
Understanding 1st & 2nd Generation Cephalosporins
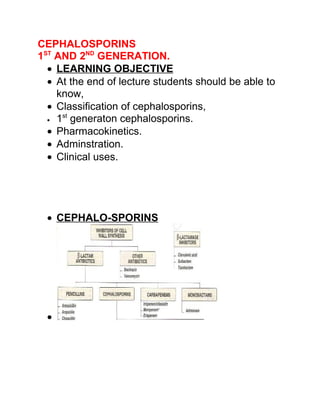
- 1. CEPHALOSPORINS 1ST AND 2ND GENERATION. • LEARNING OBJECTIVE • At the end of lecture students should be able to know, • Classification of cephalosporins, st • 1 generaton cephalosporins. • Pharmacokinetics. • Adminstration. • Clinical uses. • CEPHALO-SPORINS •
- 2. • • CEPHALO-SPORINS • First discovered in 1945 from a Cephalosporium fungi. • The cephalosporins (CS) are derivatives of 7- aminocephalo-sporanic acid. • They are B-lactam antibiotics • that are closely related both structurally and functionally to the penicillins. • CEPHALO-SPORINS • Most CS, are produced serine-synthetically by the chemical attachments of side chains to 7- aminocephalosporanic acid. • CSs and cephamycins have the same mode of action as the penicillins & are effected by the same resistance mechanisms, but they tend to be more resistant than the penicillins to B- lactamases.
- 3. • CEPHALO-SPORINS • Commercial drugs derived semi-synthetically. • Reasons for synthetic modification include: o Increased acid stability o Improved pharmacokinetics (oral absorption) o Broaden antimicrobial spectrum o Increased activity (decreased resistance due to destruction) o Improved penetration o Increased receptor affinity o Decreased allergenicity o Increased tolerance due to parenteral administration • ANTI-BACTERIAL SPECTRUM • Cephalosporins have been classified as first, second or third generation(now- a-days 4th generation), largely on the basis of bacterial susceptibility patterns and resistance to B- lactamases. • They are ineffective against methicillin-resistant staphylococcus • (MRSA), listeria monocytogenes, clostridium difficle and the enterococci. • NAME OF CEPHALOSPORINS • G1
- 4. o PO: Cephalexin, Cephradine, Cephadroxil o Parenteral: Cefapirin, Cefazolin • G2 o PO: Cefaclor, Loracarbef, Cefprozil, Cefuroxime o Parenteral:Cefmetazole,Cefotetan,Cefoxitin. Cefonacid, Cefamandol. • G3 o PO: Cefpodoxime, Cefixime, Cefdinir, Ceftitbuten o Parenteral: Cefotaxime, Ceftizoxime, Ceftriaxone, Ceftazidime, Cefaperazone • G4 - Cefepime • FIRST GENERATION • They act as penicillin “G” substitute that are resistant to the staphylococcal penicillinase • (B-lactamase). • FIRST GENERATION • First generation displays great activity against gram positive organisms, but have some activity against gram negative organisms → e.g proteus mirabilis,E. coli and klebsiella pneumonia. • First generation having poor C.S.F Penetrability and narrow spectrum. • SECOND GENERATION
- 5. • They are more effective against gram negative and less effective against gram positive organisms as compare to first generation. • The second generation CSs display greater activity against 3 additional gram negative organism, Homophilus influenzae, some Entrobactera-erogenes and some neisseria species. • Having un-reliable C.S.F penetrability and intermediate spectrum. • Transition from first generation to third generation agents • Transition from first generation to third generation agents reflects o 1)Broadening of the Gram (-) organism spectrum o 2)Loss of efficacy against Gram (+) organisms o 3)Greater efficacy against resistant organisms (but increased cost) • PHARMACOKINETICS • ADMINISTRATION • All the CS (except cephalexin, cephradine and cefiximine) must be administered
- 6. intravenously because of poor oral absorption. • DISTRIBUTION • All of these antibiotics distribute very well into body fluids. • However, adequate therapeutic levels in the C.S.F, regardless of inflammation, are achieved only with the 3rd generation CS, because most CS do not penetrate into the C.S.F. • FATE • Biotransformation of Cs by the host is not clinically important. • Elimination occurs through tubular secretion &/ OR glomerular filtration,thus doses must be adjusted in the case of severe renal failure to guard against accumulation & toxicity. • SIDE EFFECTS • Allergic manifestation. • Disulfiram like effect when patient also takes alcoholic drinks(cefamandole & cefoperazone. as seen in alcoholics.Increased hangover effect of ethanol B/C aldehyde dehydrogenase is blocked) • 3)Hypoprothrombinemia & Bleeding disorders • TOXICITY:Local irritation can produce severe pain after I/M injection & thrombophlebitis after I/
- 7. V injection.Renal toxicity,including interstitial nephritis & even tubular necrosis,has been demostrated & has caused the withdrawal of drug. • 5)SUPERINFECTION:Mostly through 2nd generation Cephalosporins. • CLINICAL USES OF CEPHALOSPORINS • Cephalosporins have been shown to be effective as therapeutic and prophylactic agents • Cephalosprins with or without aminoglycosides are used for serious infections caused by haemophilus, klebsiella , enterobacter , and serratia species . • Cephalosporins can be used as an alternative to peniciins for a variety of infections especially streptococcal and staphylococcal infection where patients are not able to tolerate penicillin . • CLINICAL USES OF CEPHALOSPORINS • First generation cephalosporins have been used for prophylaxis during and after surgery . • However, they are rarely the drug of choice for any infection .
- 8. • Oral drug may be used for the treatment of UTIs , for minor staphylococcal lesions , or for soft tissue abscess and cellulitis . • CLINICAL USES OF CEPHALOSPORINS • For surgical prophylaxis , first generation cephalosporins can be administered as they penetrate most tissues well and are drugs of first choice . • Second and third generation cephalosprons offered no advantage for surgical prophylaxis . • Infection with anaerobes are preferably treated with a combination of anti biotic because in these infection aerobic organisms are also present . • Cefoxitin and cefotetan are quite effective against anaerobes and can be considered for monotherapy against certain organism. • CLINICAL USES OF CEPHALOSPORINS • H. Influenzae infection can be treated both by second OR third generation cephalosporins .However,because of their penetration to the CNS ,3rd generation CS (except cefoperazone) are effective in meningitis caused by meningococci , pneumococci , and H. Influenzae and susceptible gram negative bacilli.
- 9. • Treatment with some second or third generation cephalosporins is equivalent or superior to treatment with a combination of ampicillin and chloramphenicol for meningitis caused by H. Influenzae . • THANKYOU