Downloaded 127 times
















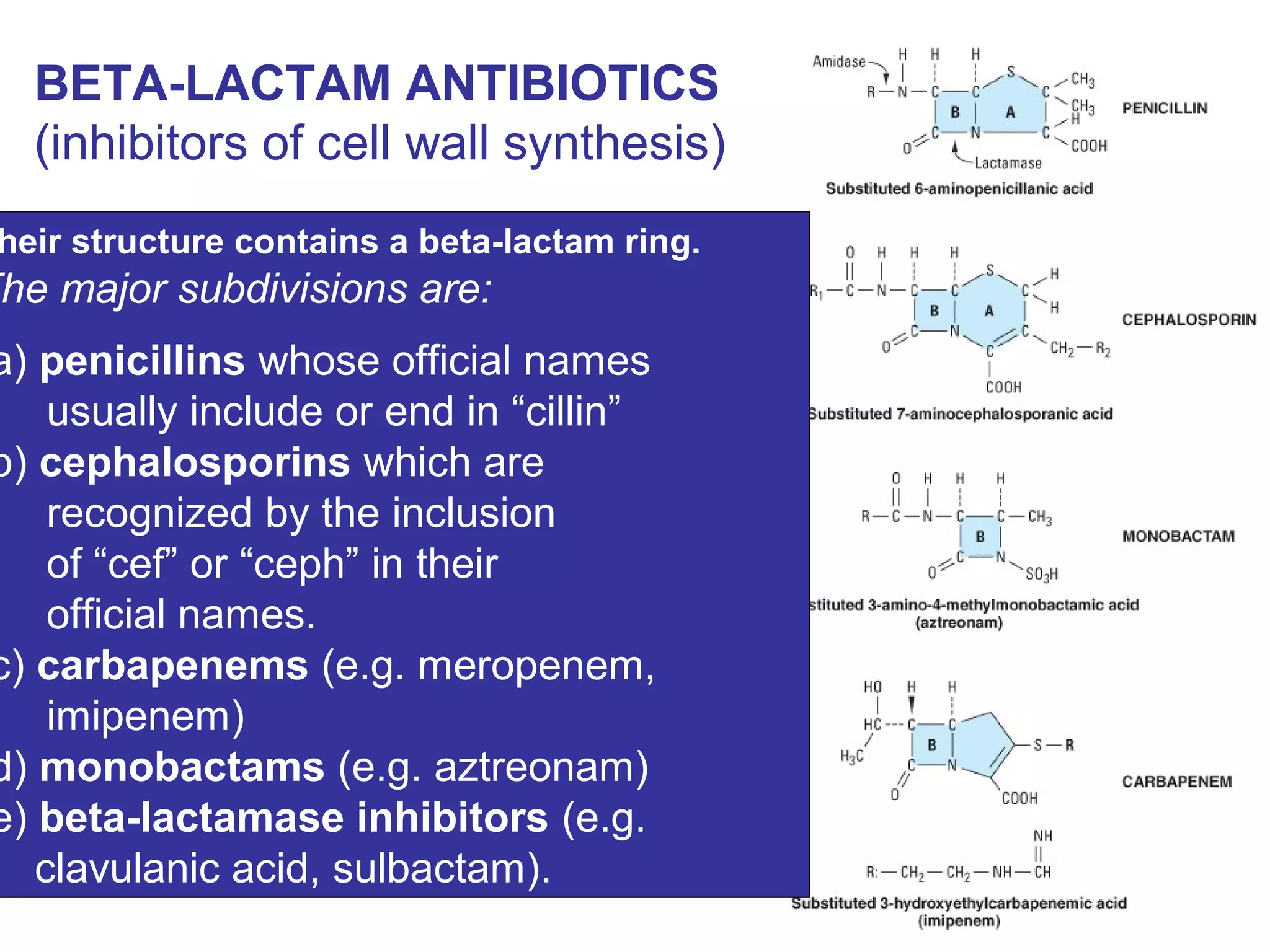































































This document discusses beta-lactam antibiotics, including penicillins. It describes how penicillins work by inhibiting bacterial cell wall synthesis through binding to penicillin-binding proteins. This prevents cross-linking of peptidoglycan and kills bacteria. It classifies penicillins as narrow spectrum (natural penicillins) or broad spectrum (aminopenicillins, antipseudomonal penicillins). Common adverse effects include allergic reactions and disruption of normal gut flora. Resistance can develop through plasmids transferring resistance genes.























































































