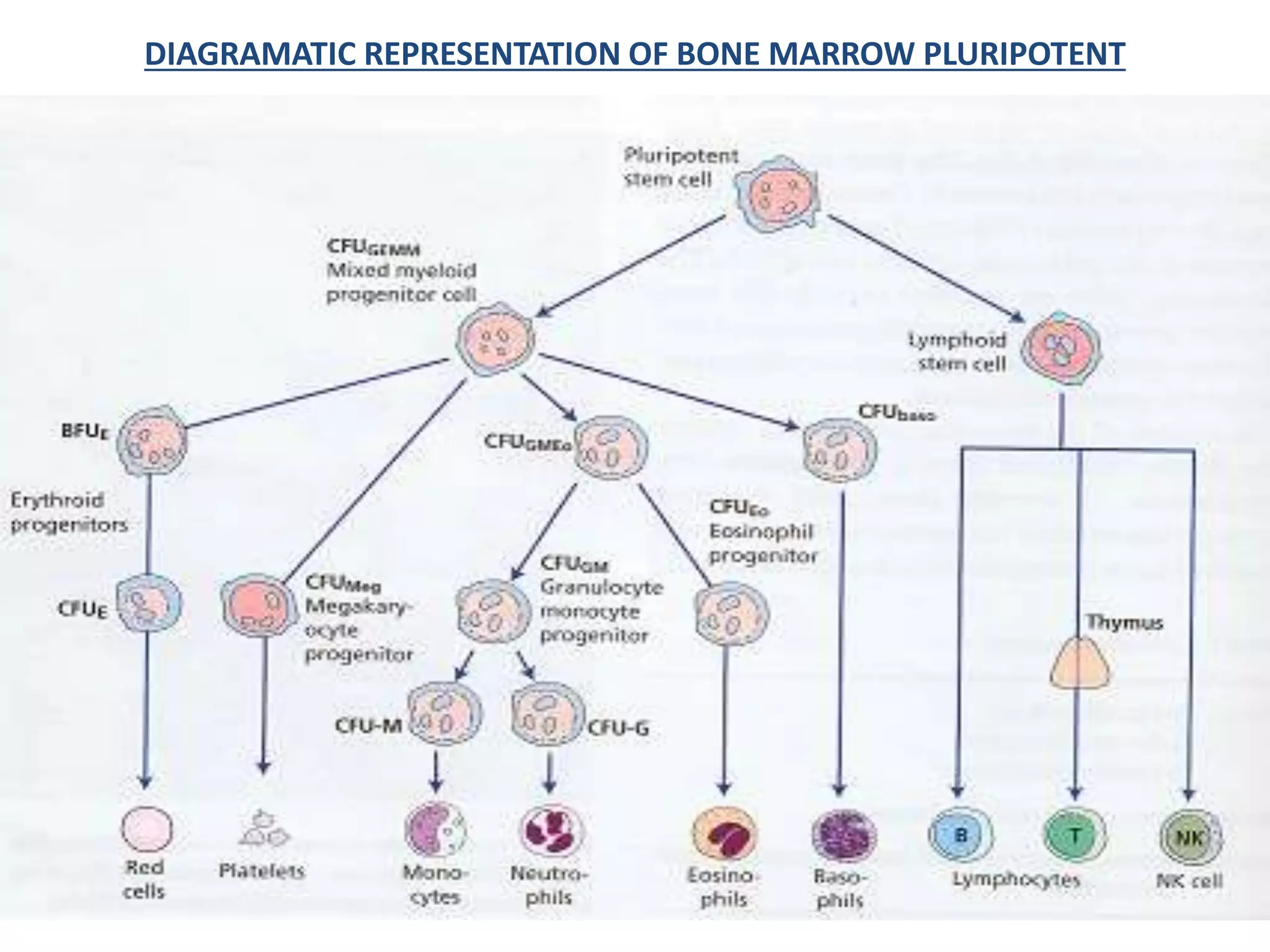
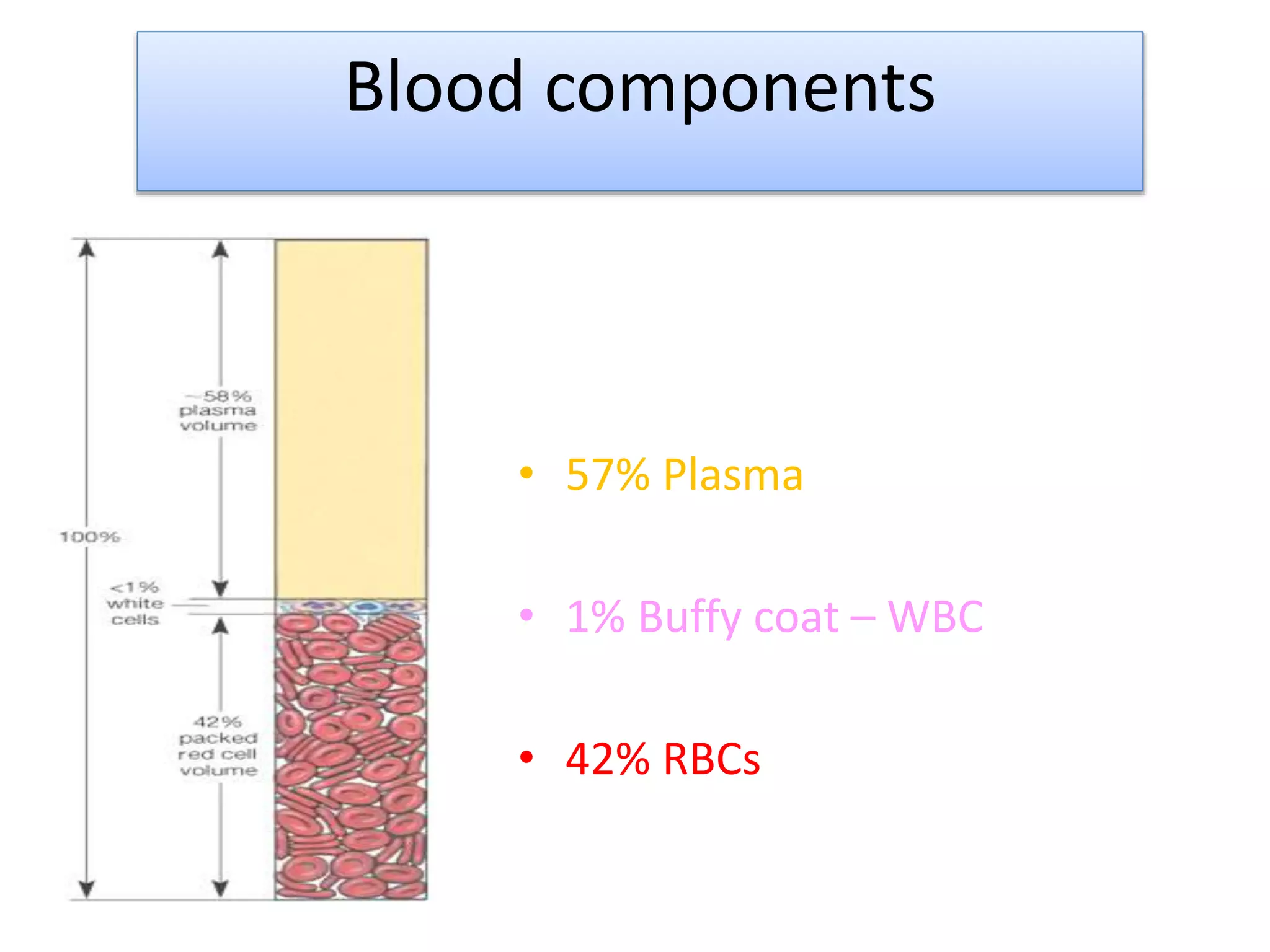
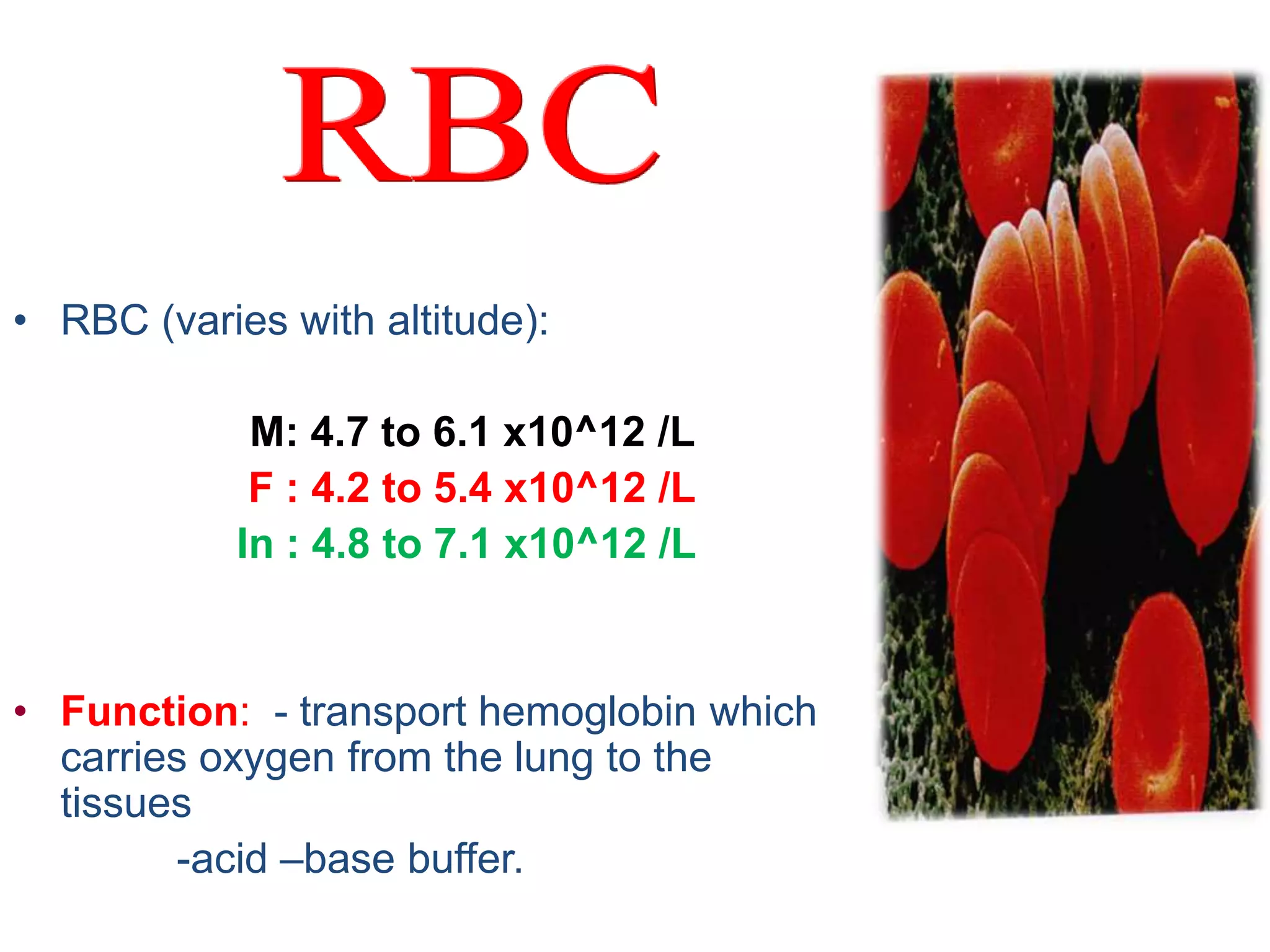
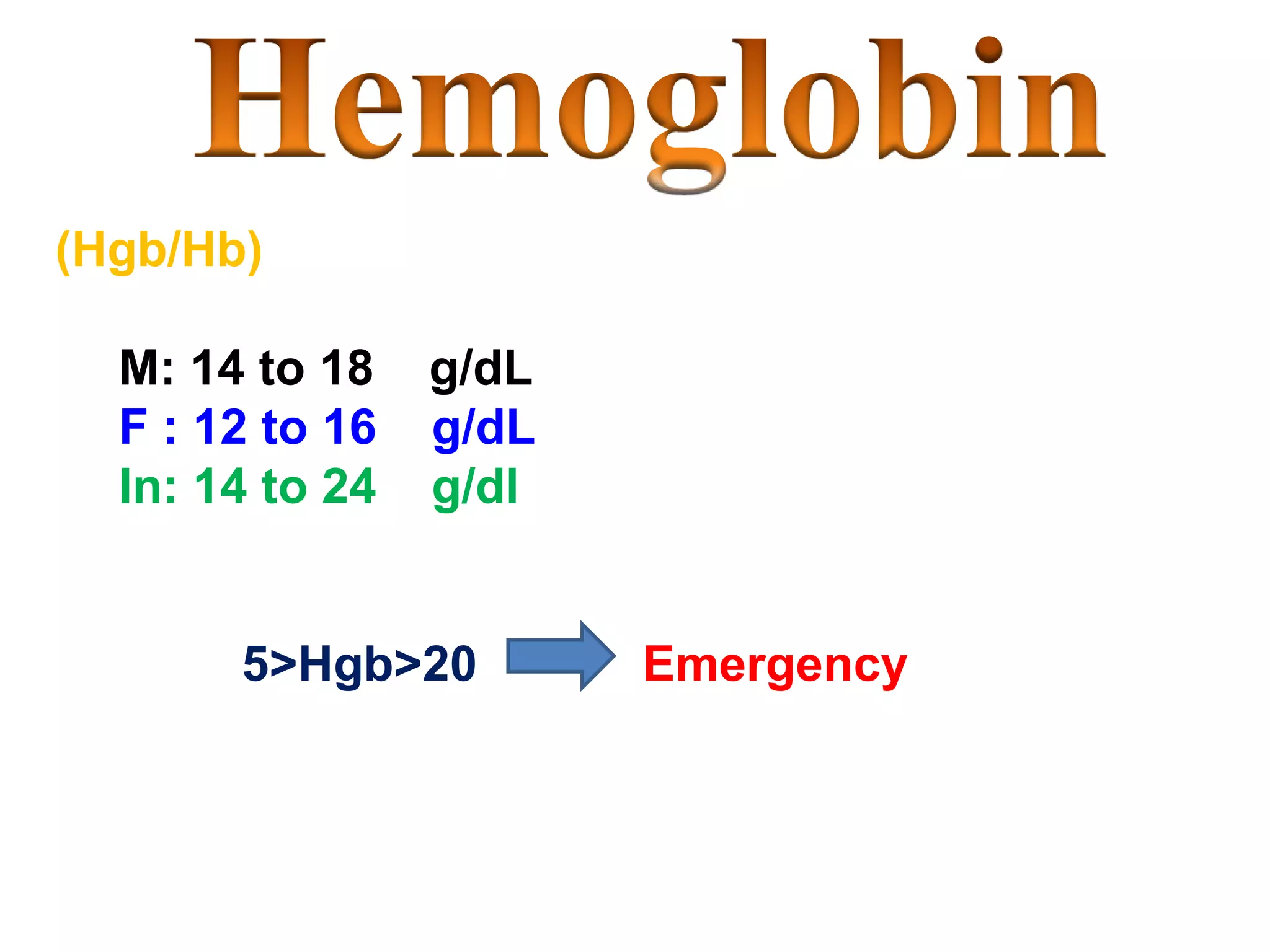
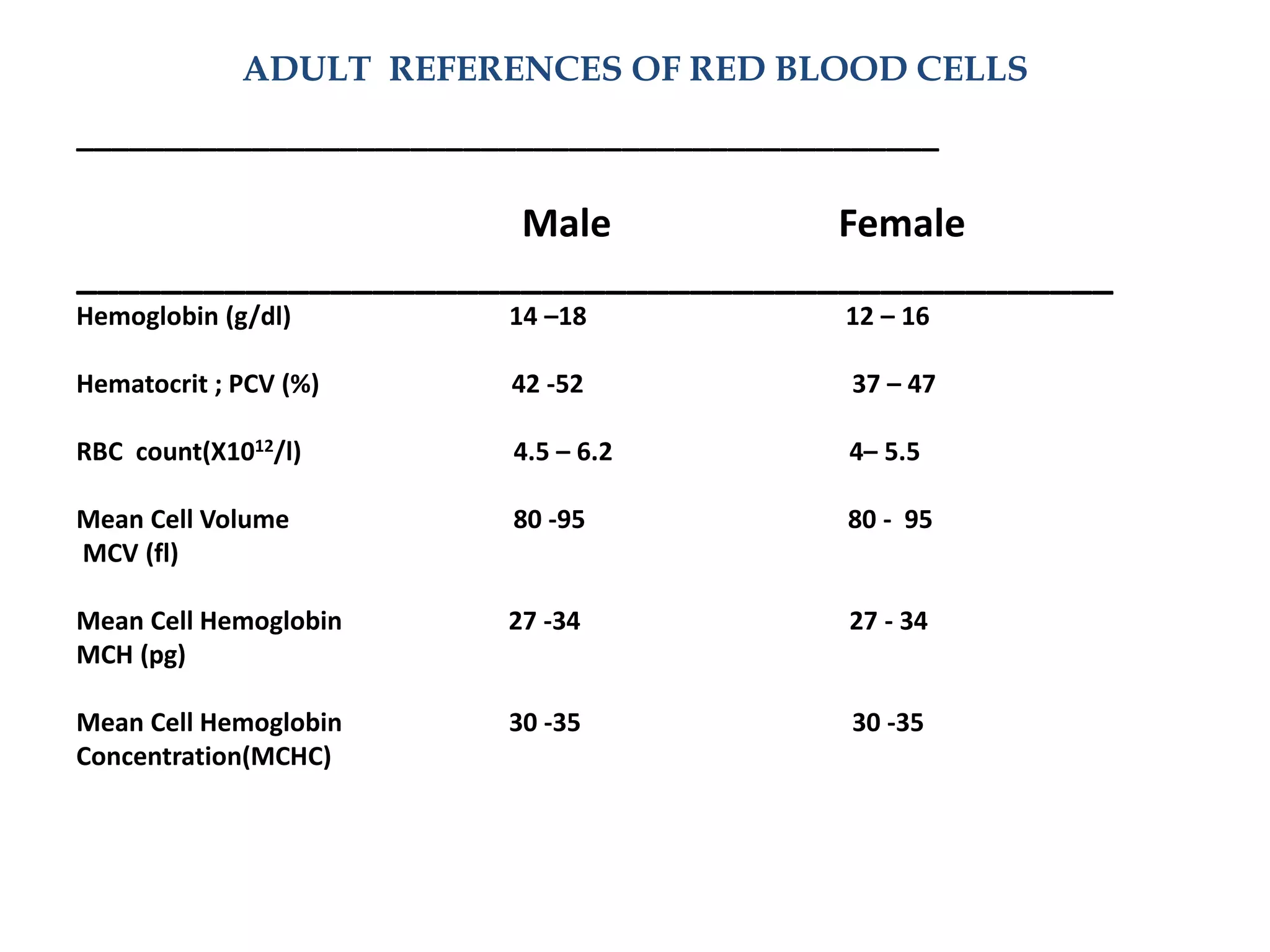
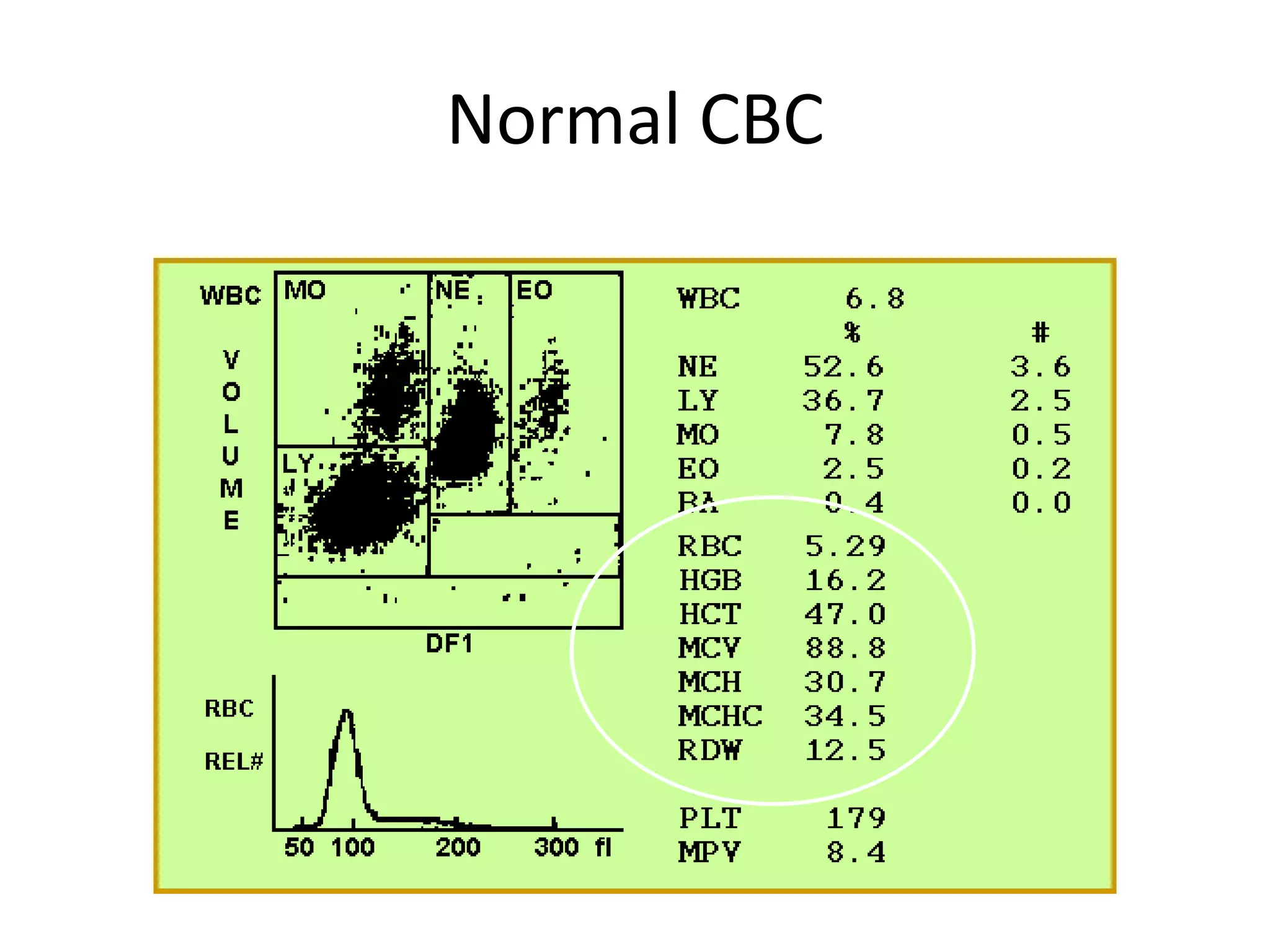
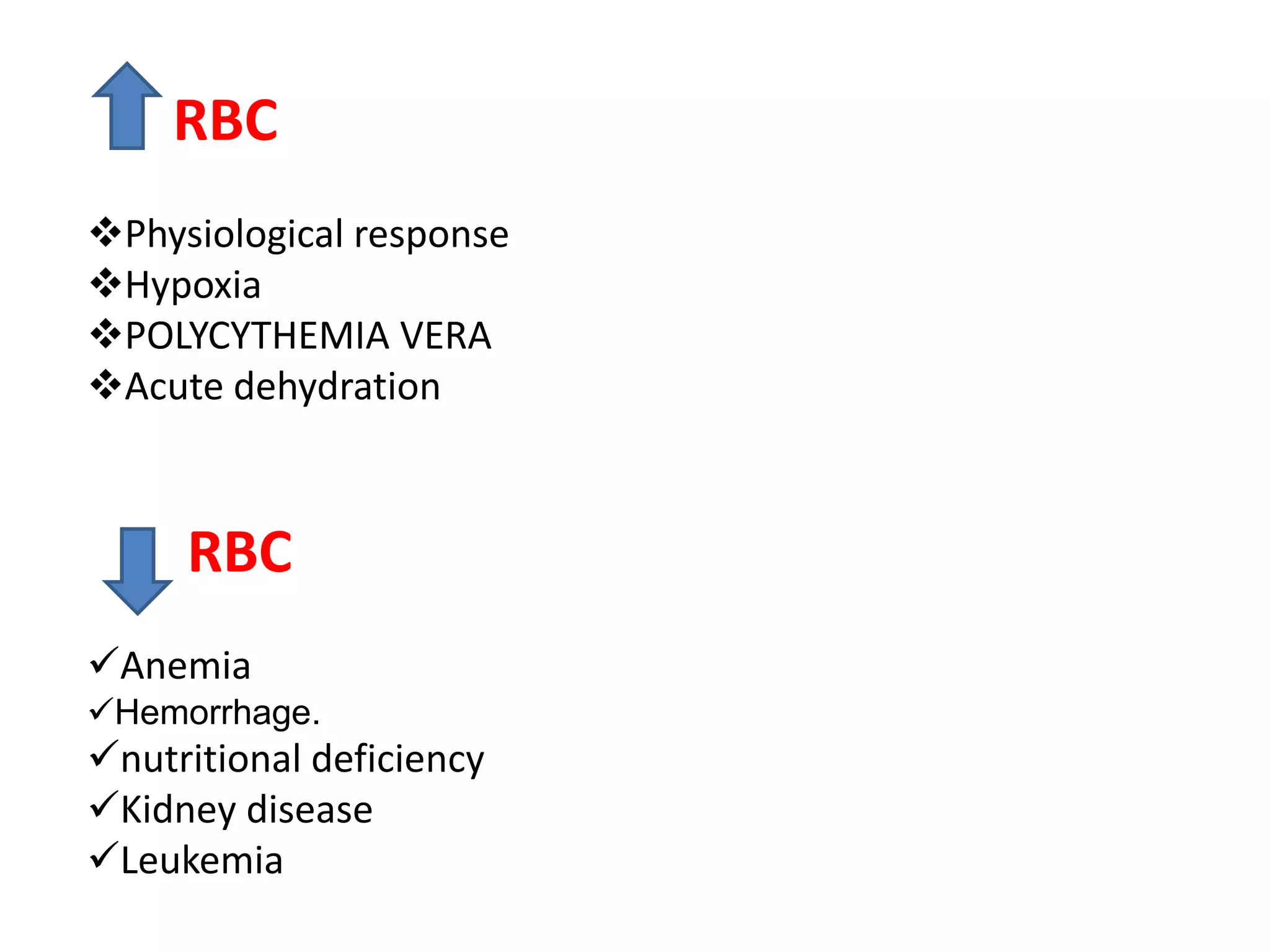
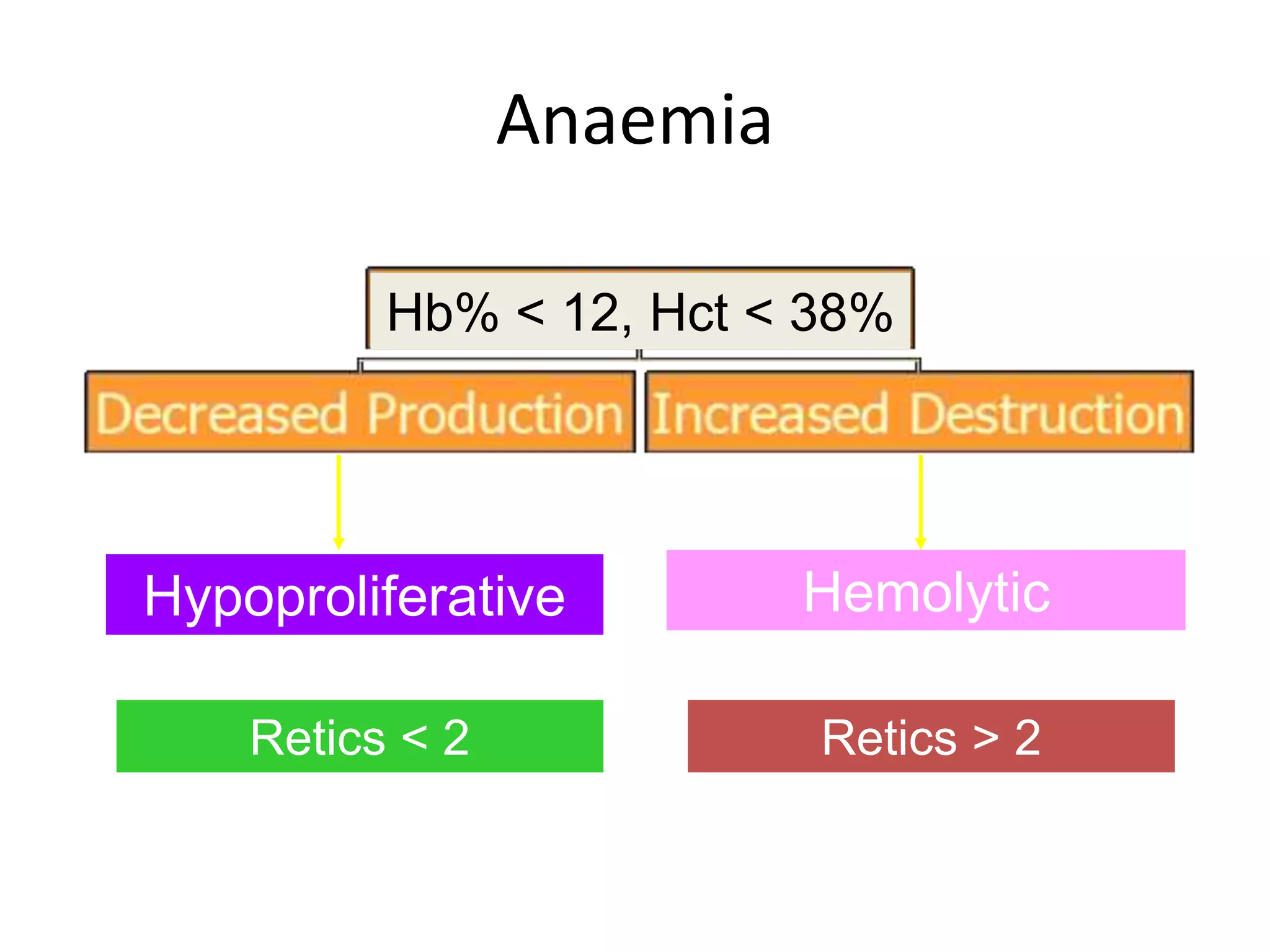
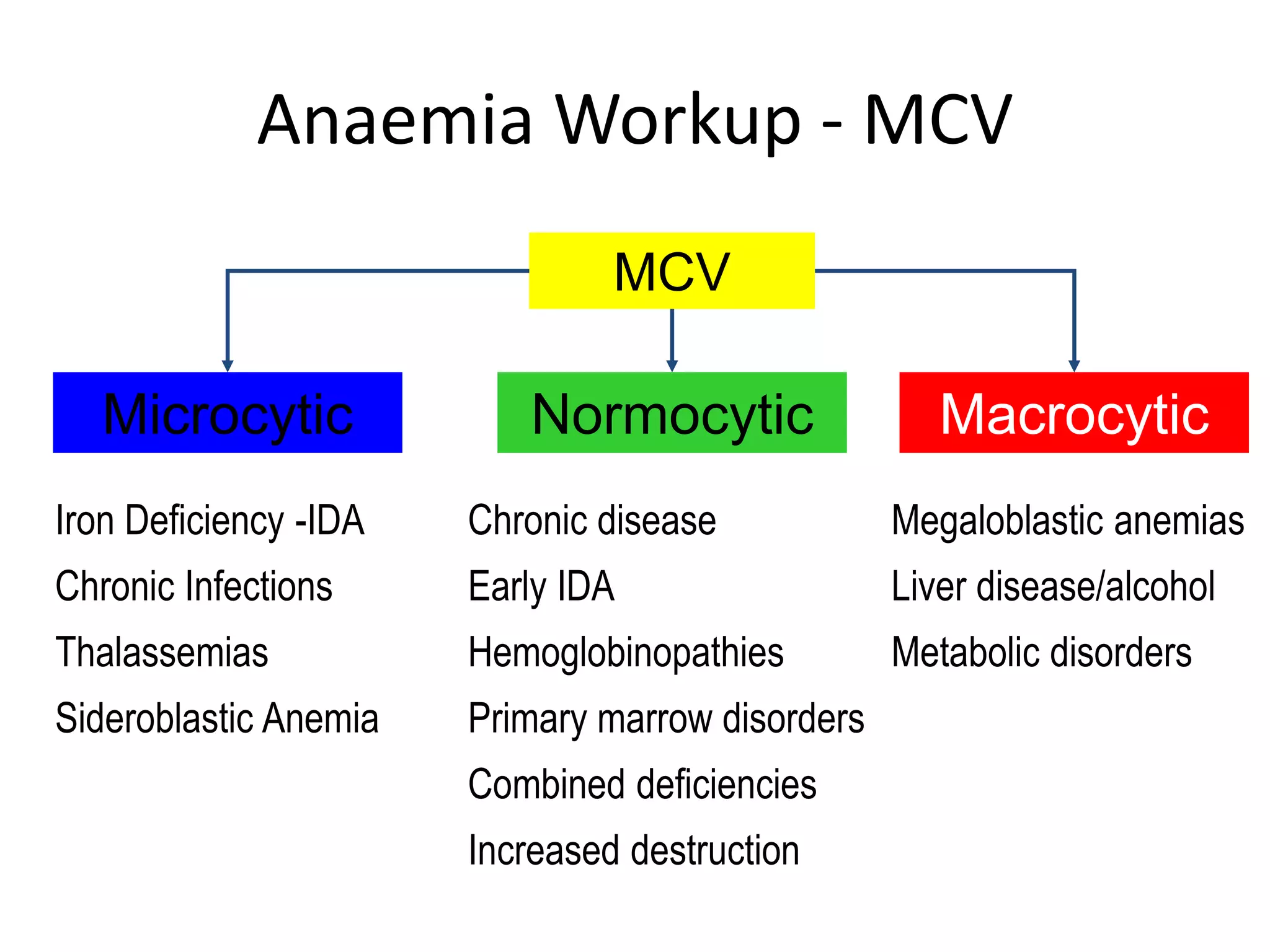
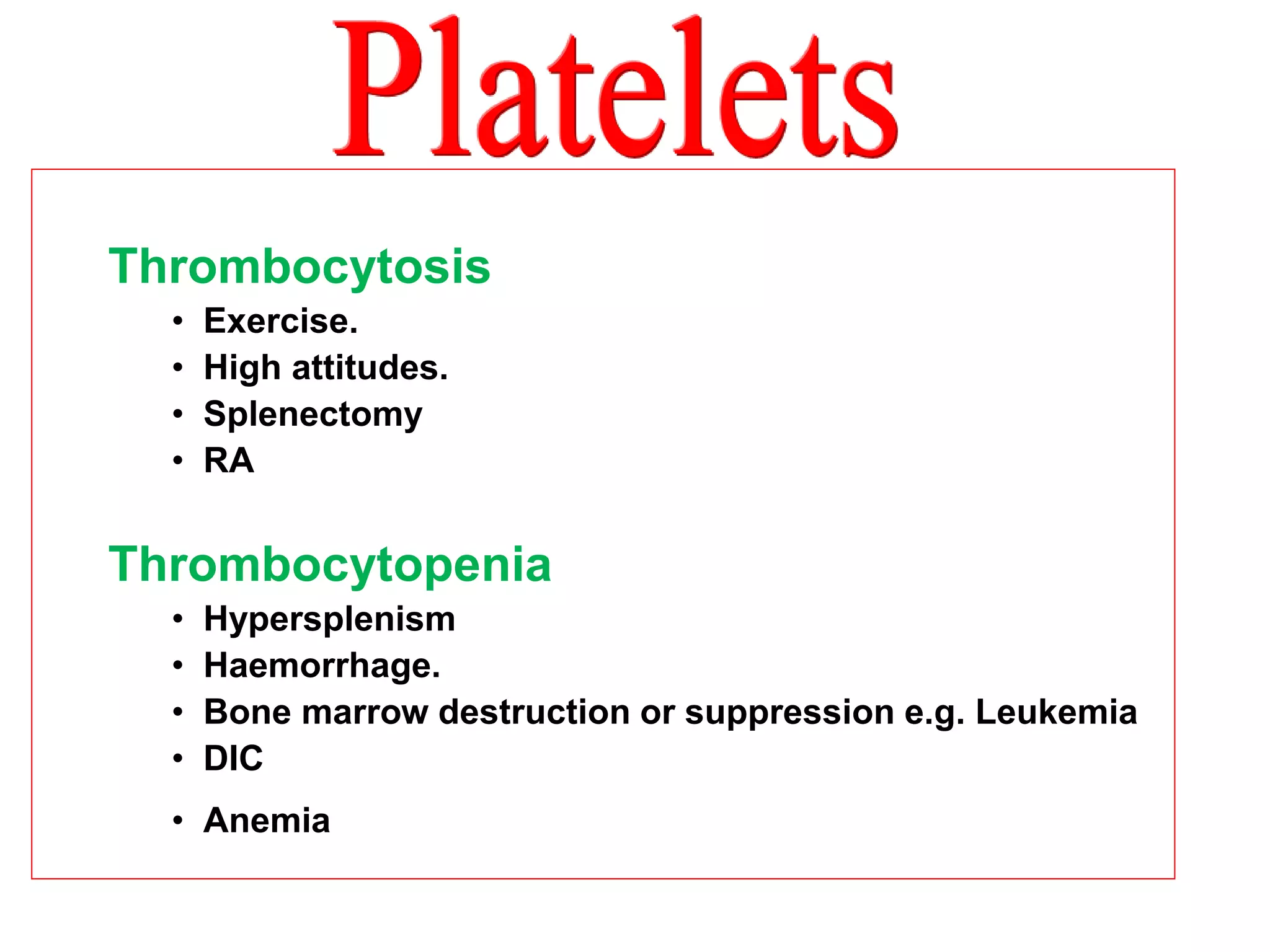
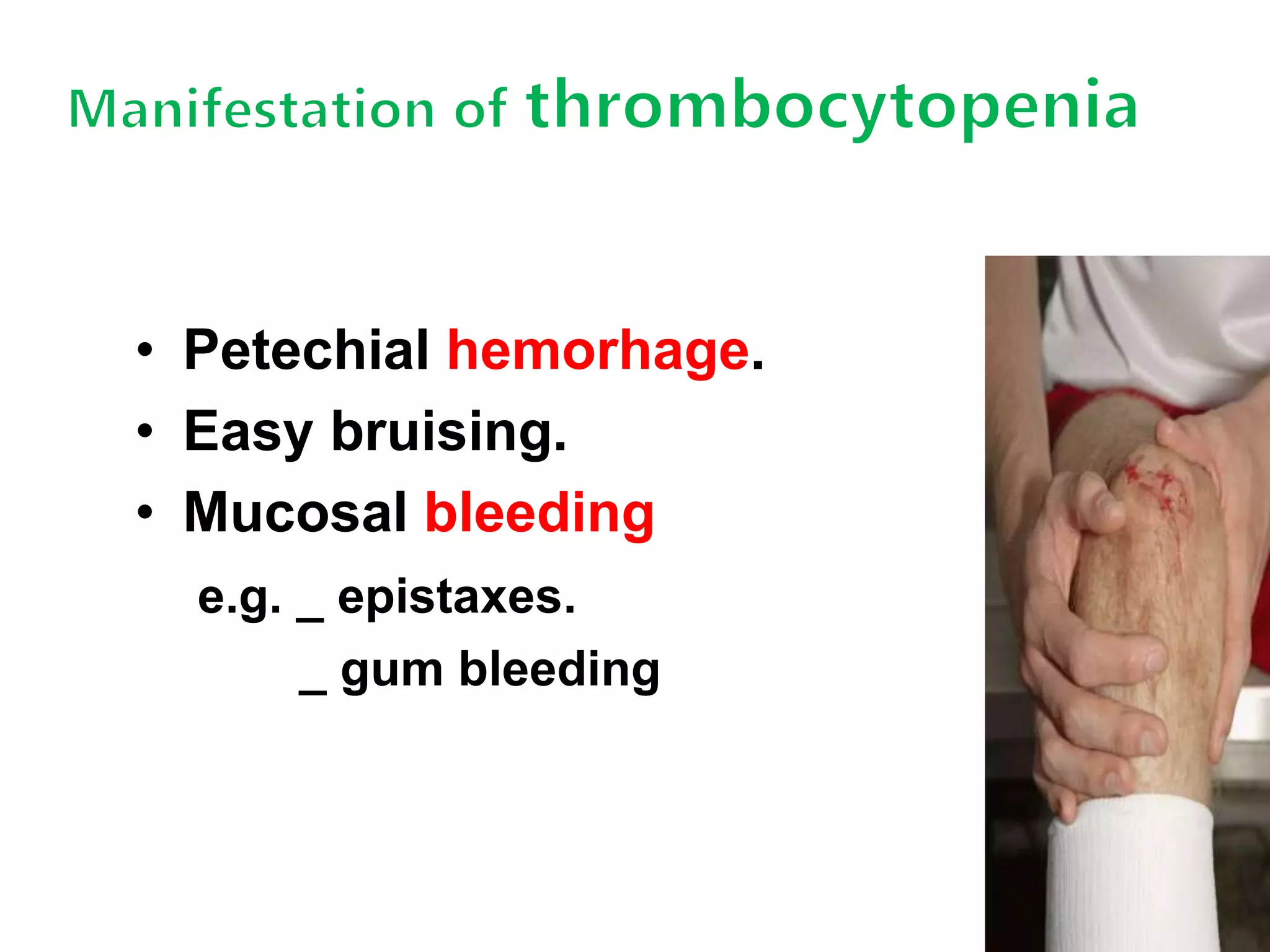
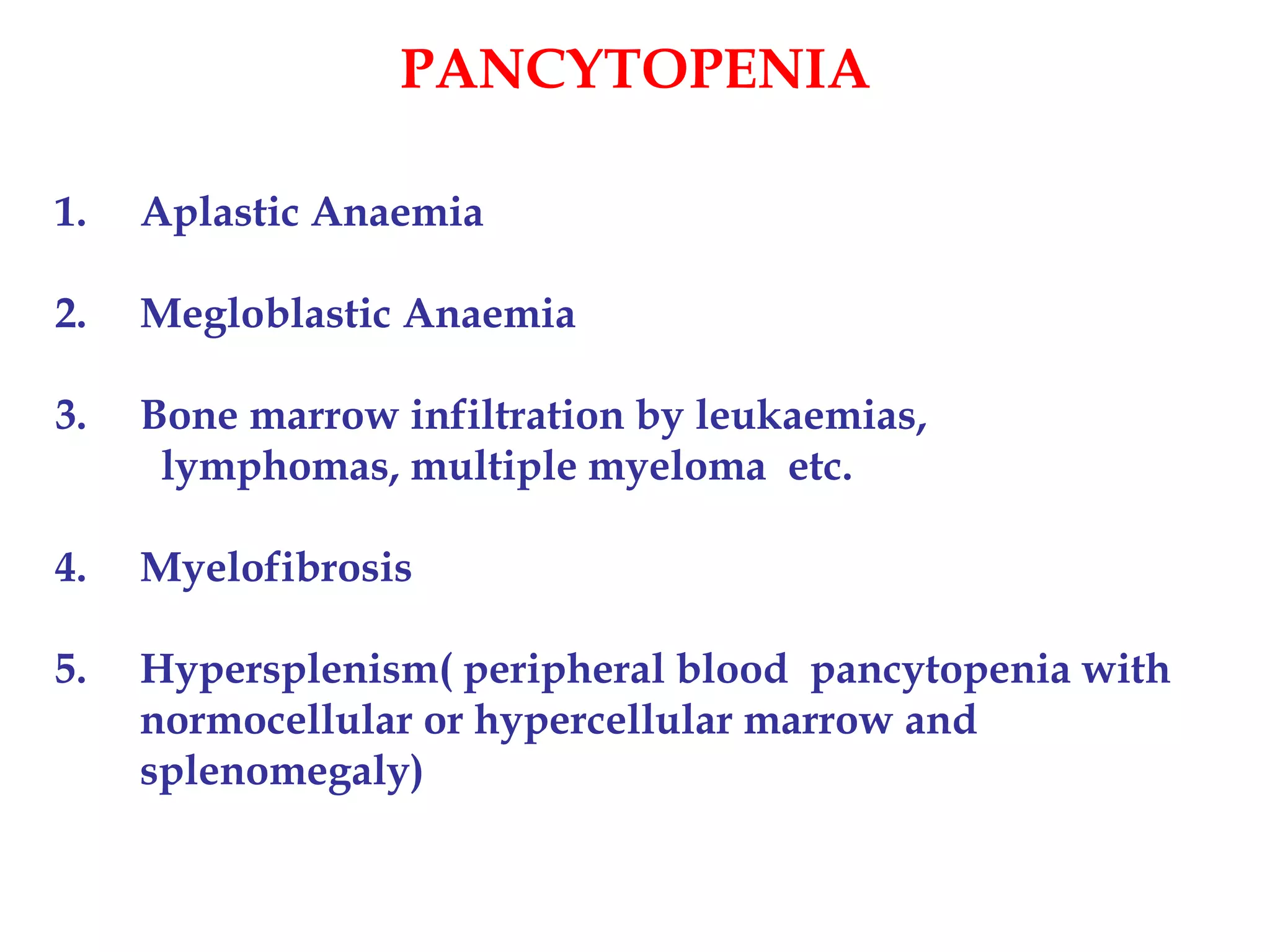
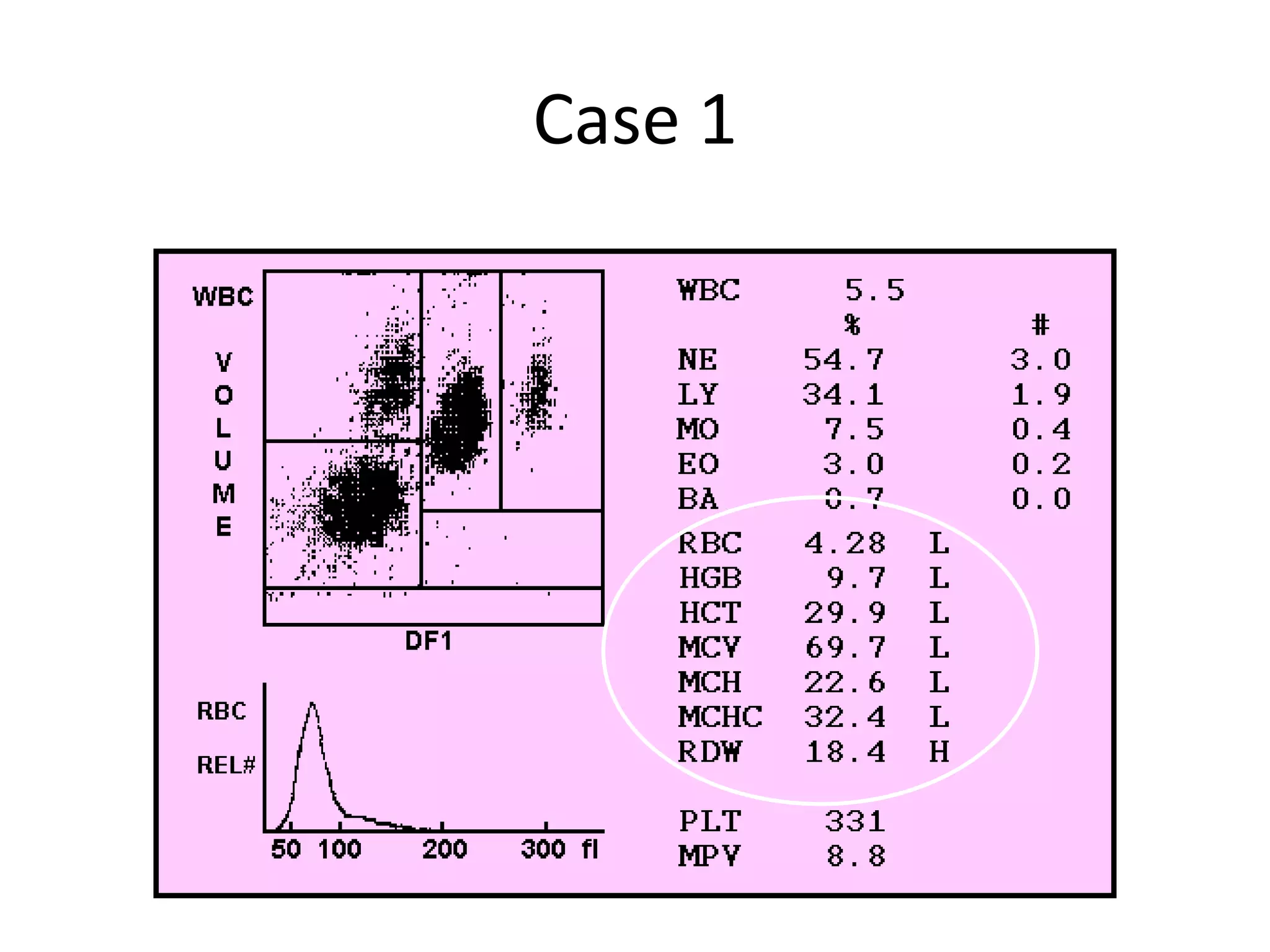
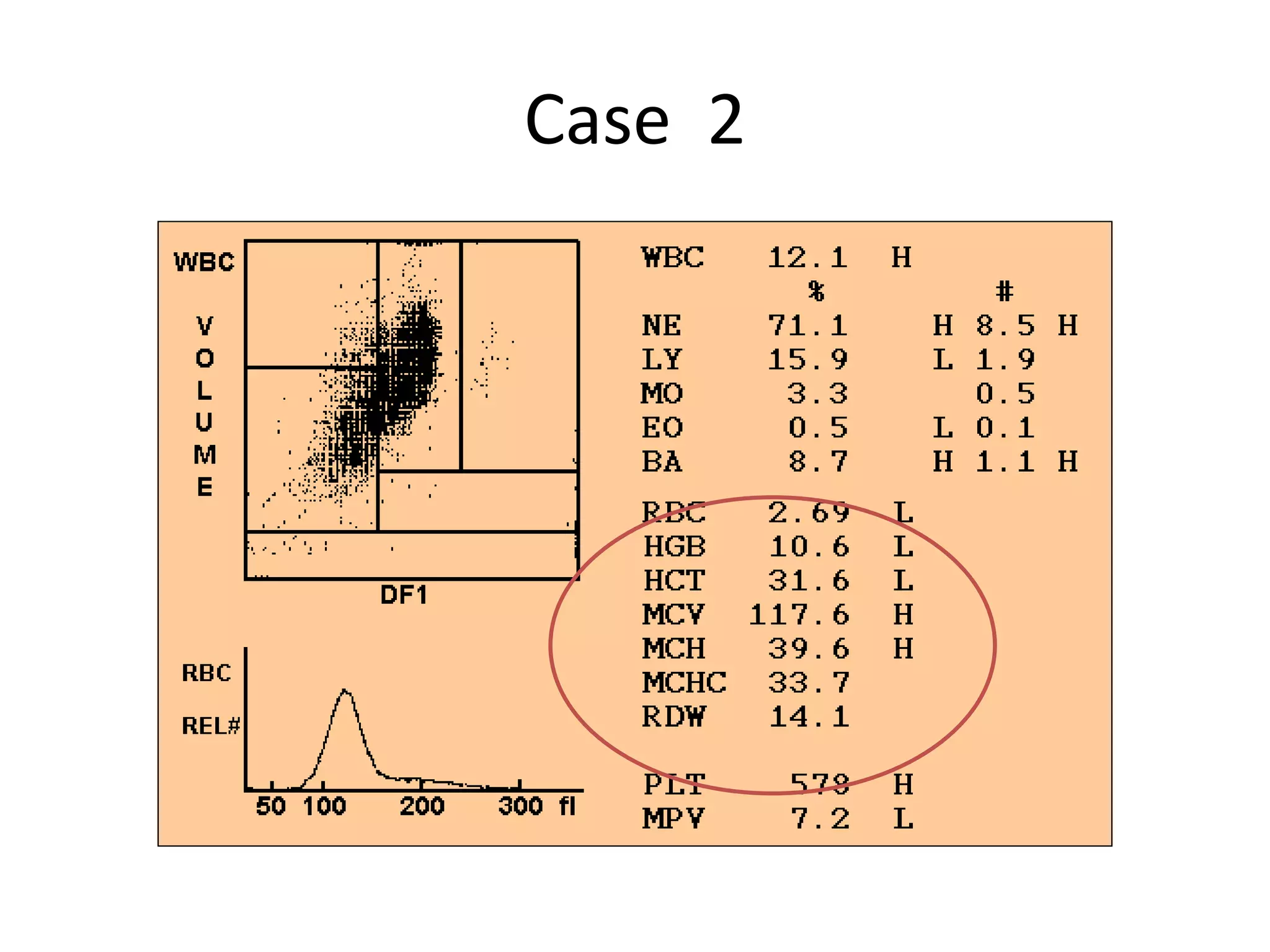
This document provides information about components of a complete blood count (CBC) test and their normal ranges. It discusses red blood cells, white blood cells, platelets, hematocrit, hemoglobin and other components. Abnormal results are explained, such as anemia, leukocytosis, thrombocytopenia. Causes of abnormalities in each component are outlined, including infections, deficiencies, diseases. Interpretation of CBC can provide clues to underlying bone marrow or blood disorders.