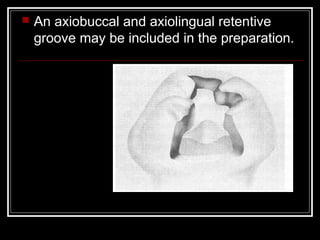
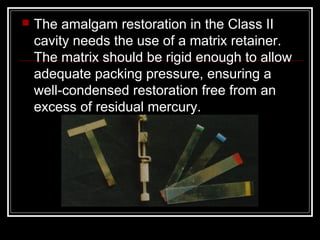
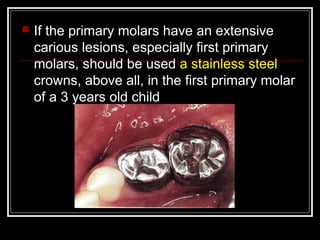
Downloaded 15 times
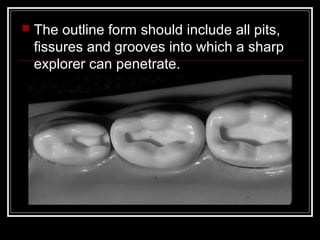
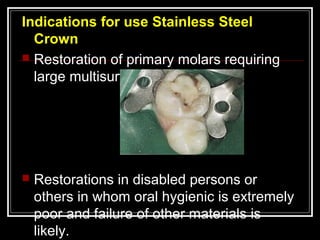

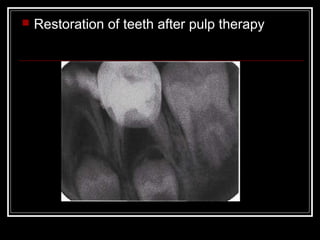

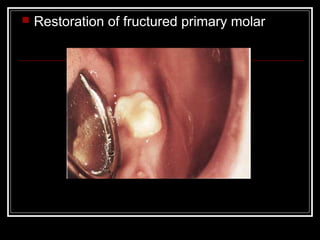


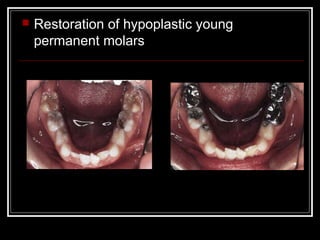
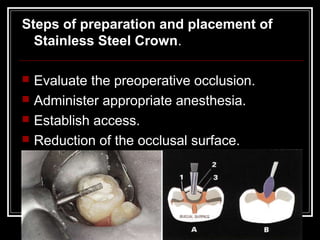

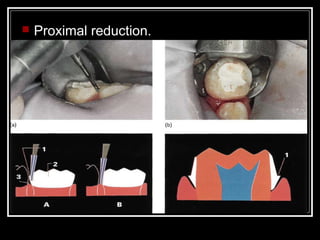
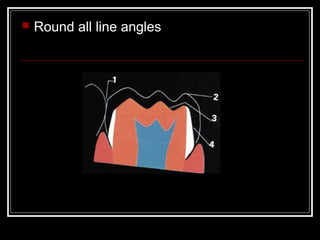
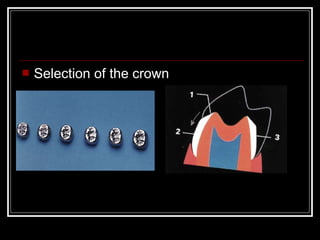

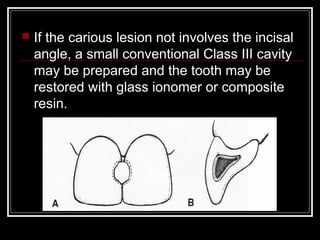
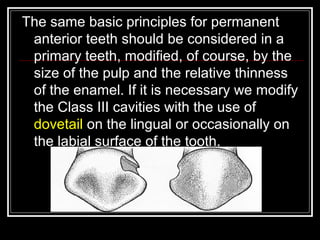
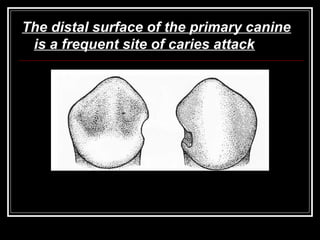
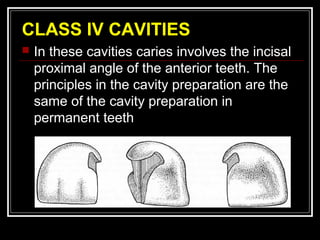
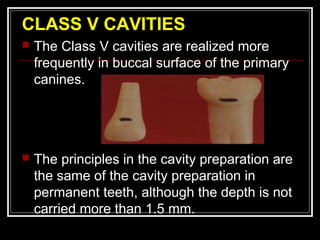
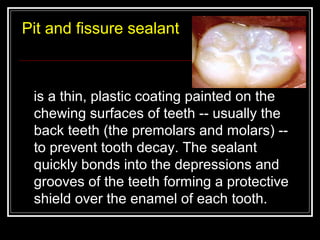

The document discusses cavity preparation in primary teeth. It outlines the basic principles of Black's cavity preparation and describes how to prepare cavities for each class: Class I cavities involve occlusal surfaces, Class II cavities involve occlusal and proximal surfaces, Class III cavities involve proximal surfaces of anterior teeth, Class IV cavities extend into the proximal incisal angle, and Class V cavities involve cervical lesions. Stainless steel crowns are recommended for restoring teeth with large cavities or poor oral hygiene. Pit and fissure sealants can prevent cavities by protecting tooth surfaces.



































































