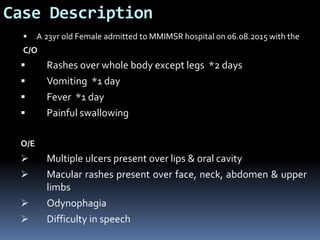
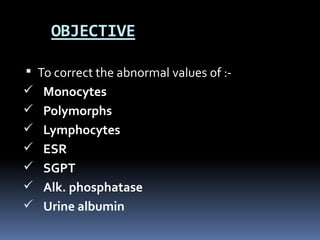
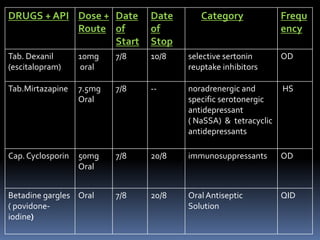
The document presents a case study of a 23-year-old female diagnosed with Steven Johnson Syndrome (SJS), a rare and serious condition typically triggered by medication or infections, marked by severe skin and mucous membrane reactions. It details her symptoms, medications, vital signs, laboratory results, and the treatment plan aimed at relieving her symptoms and preventing complications. Key medications administered include immunosuppressants, antibiotics, and anti-fungal treatments, alongside patient counseling for recovery support.