Downloaded 2,021 times














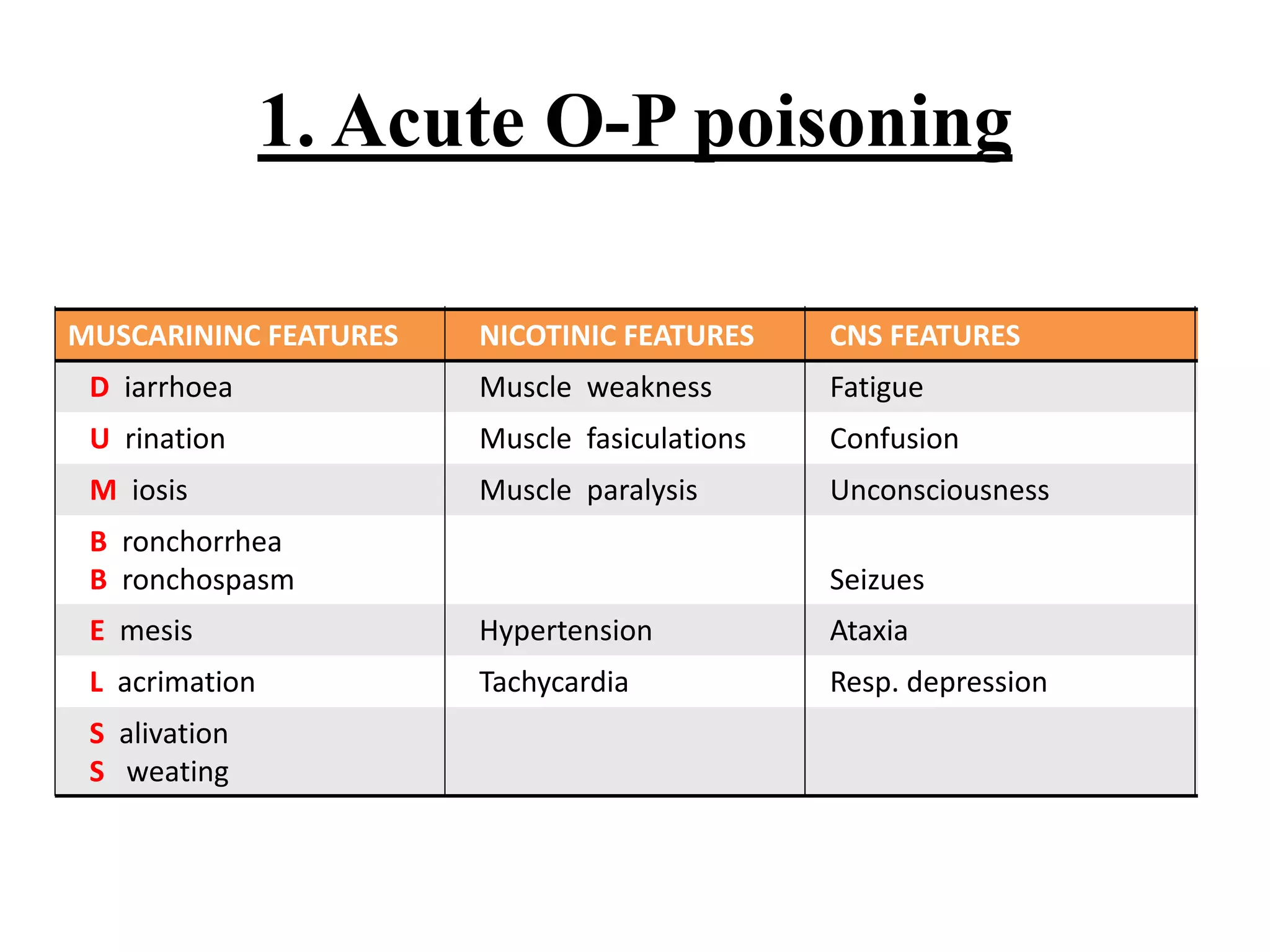

































































A 30-year-old unconscious housewife was brought to the hospital with a history of domestic violence. On examination, she had constricted pupils, low blood pressure, high blood sugar, metabolic acidosis on ABG, bradycardia on ECG, and elevated serum amylase. The diagnosis was organophosphorus poisoning based on the clinical features and laboratory findings.





















































































