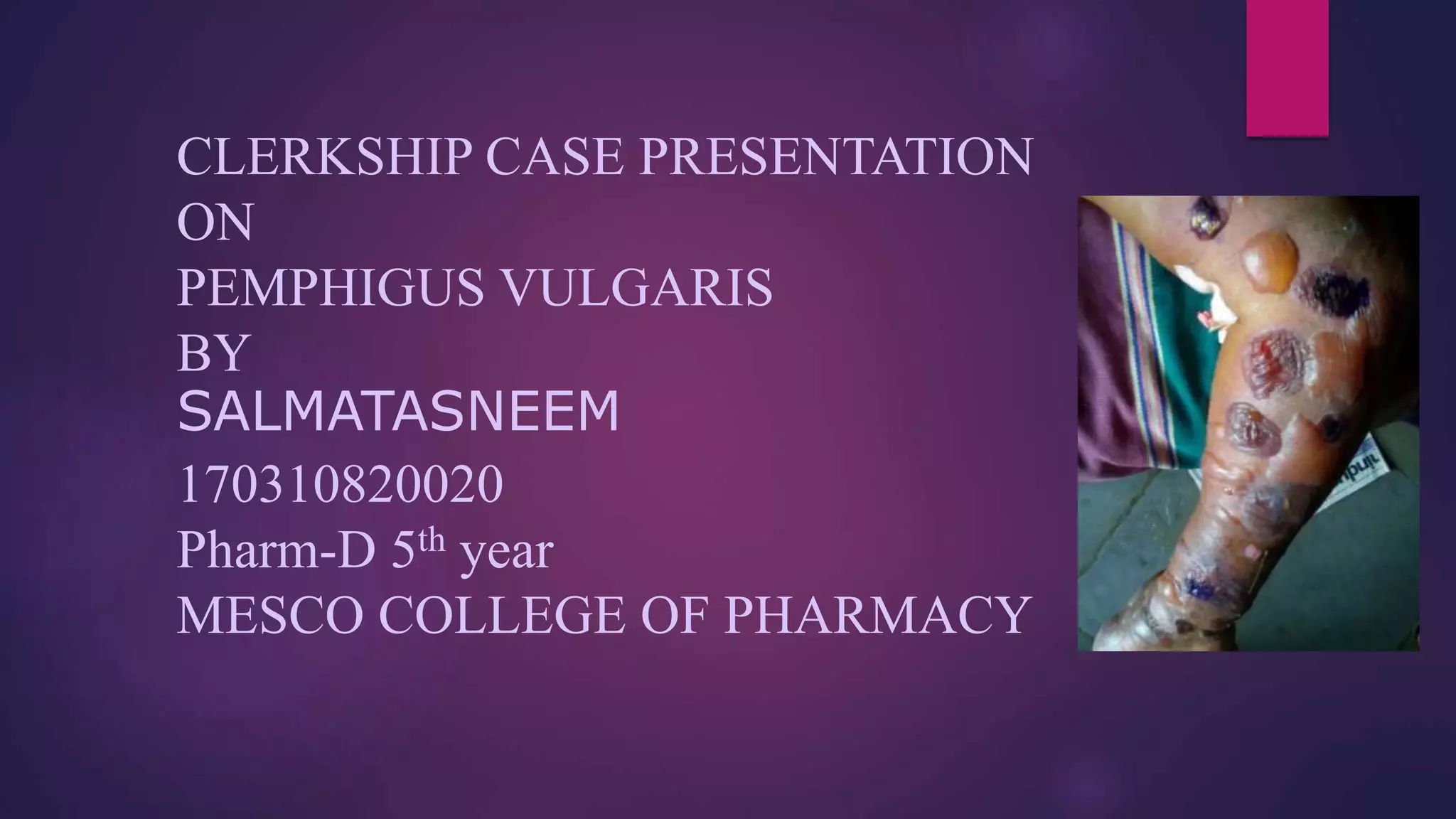
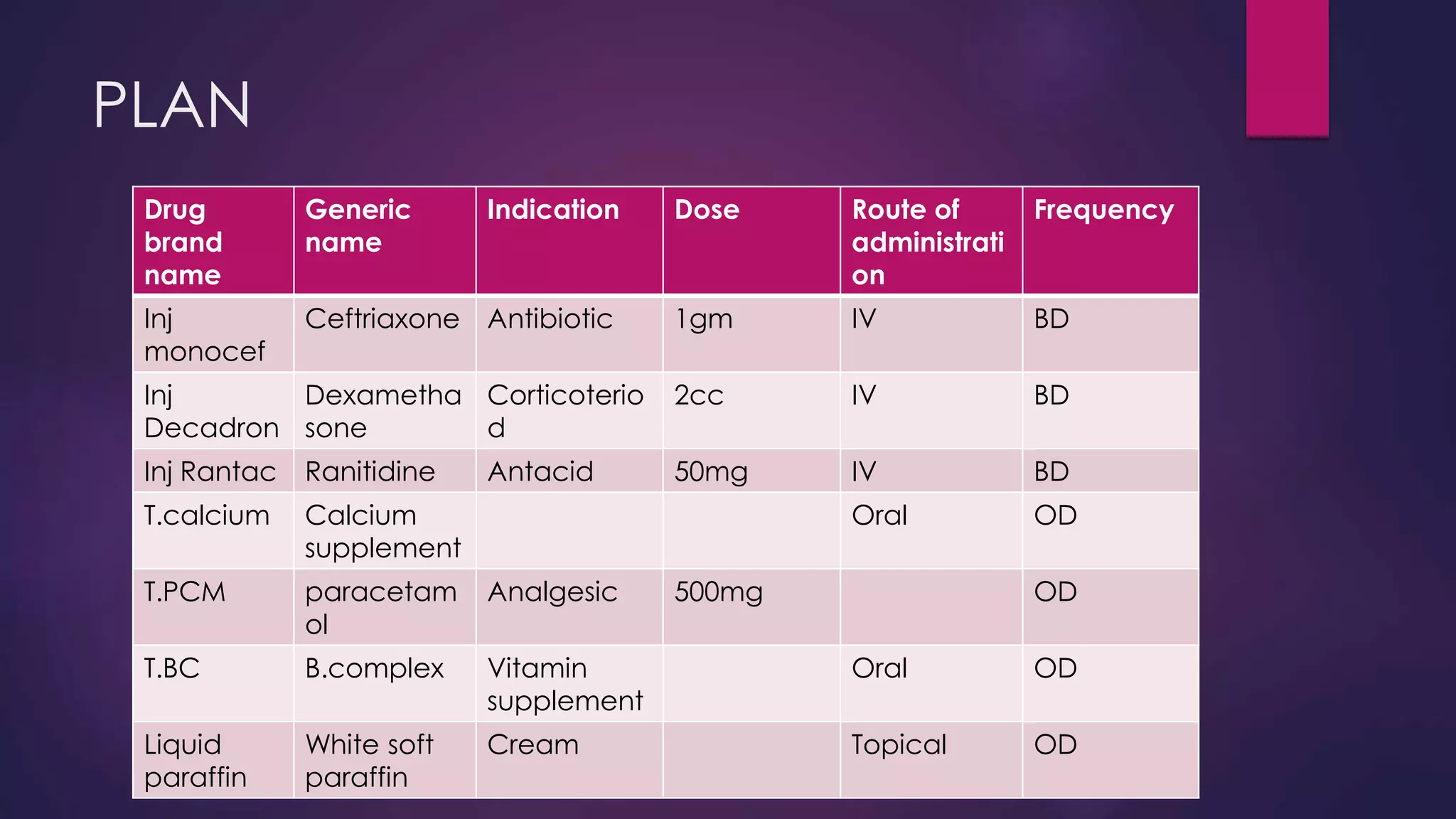
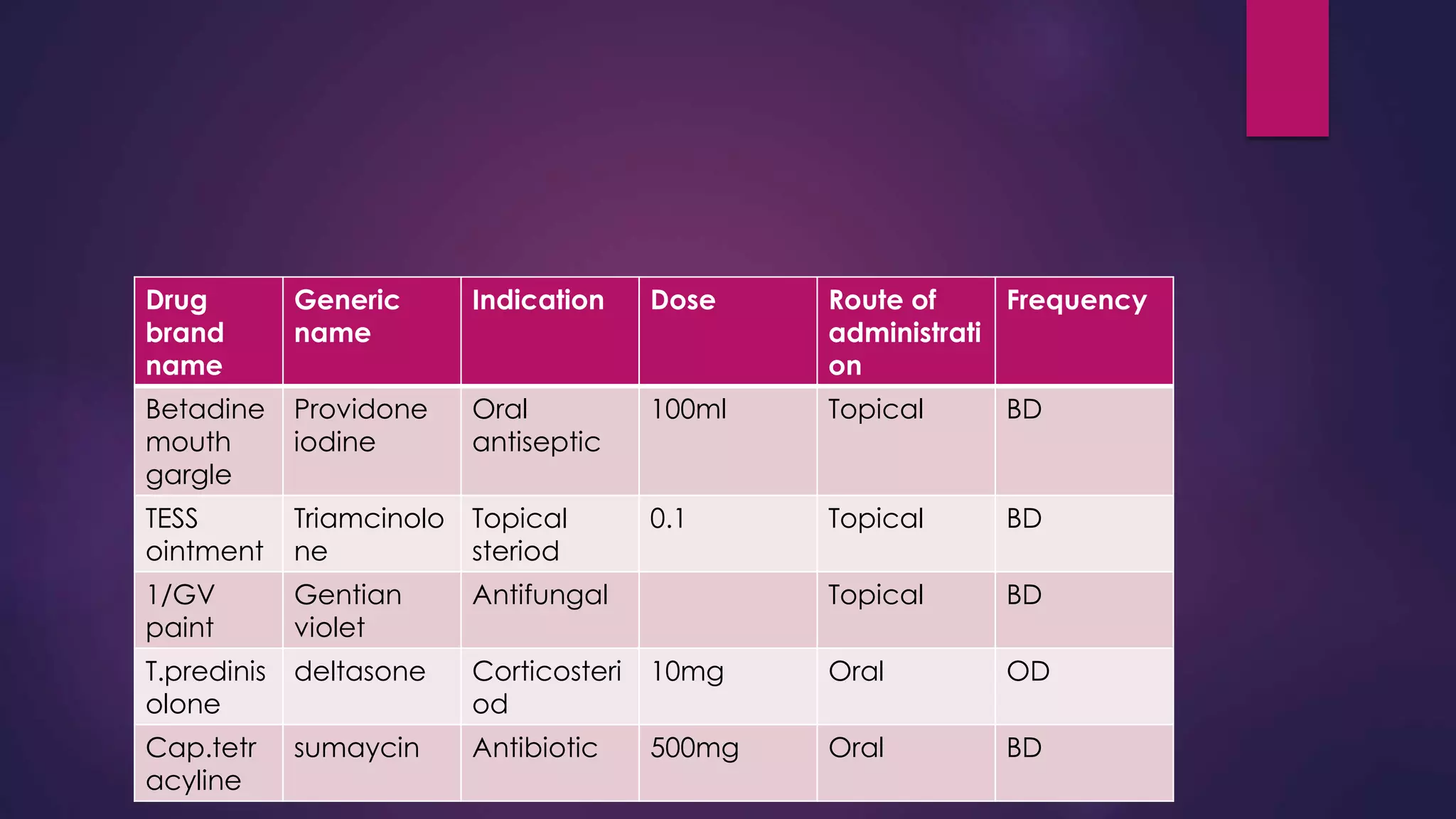
This document presents a case presentation on Pemphigus Vulgaris. The patient is an 85 year old female who presented with fluid filled lesions all over her body. On examination, multiple fluid filled blisters were seen over the limbs and trunk along with oral lesions. A skin biopsy showed features of Pemphigus Vulgaris. The patient was started on medications including antibiotics, corticosteroids, antacids and topical steroids. She was counselled about her disease, medications, lifestyle modifications and potential drug interactions.