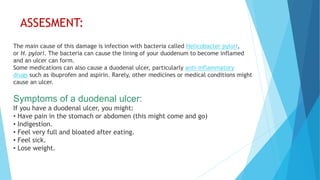
A 58-year-old male was admitted with symptoms of vomiting, abdominal pain, and no stool passage, leading to a diagnosis of perforated duodenal ulcer. He underwent laparotomy surgery on 25/10/19 and was treated with antibiotics, vitamins, and supportive care. Post-surgery, the patient was advised on dietary modifications and lifestyle changes to improve his health and avoid complications.
































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




