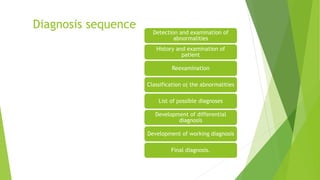
The document provides information on case history for dental treatment. It defines case history as a planned conversation between patient and clinician where the patient expresses symptoms, fears, and feelings. The objectives of case history are to establish a relationship, provide medical/dental history, and aid in diagnosis and treatment planning. Key components of case history include demographic data, chief complaint, history of present illness, medical history, dental history, family history, and personal history. Obtaining thorough case history is important for accurate diagnosis and appropriate treatment.