Download to read offline

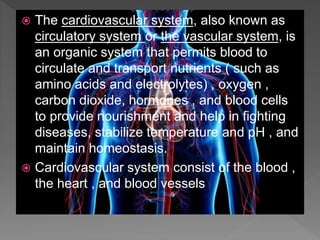























![ Hypertension (HTN or HT), also known
as high blood pressure (HBP), is a long-
term medical condition in which the blood
pressure in the arteriesis persistently
elevated.[10] High blood pressure usually
does not cause symptoms.[1] Long-term high
blood pressure, however, is a major risk
factor for several disease like heart failure .
Stroke etc.](https://image.slidesharecdn.com/cardiovascularsystem-180911082856/85/Cardiovascular-system-34-320.jpg)
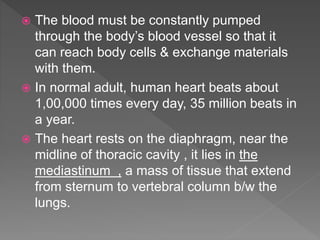
![ Heart arrhythmia (also known
as arrhythmia, dysrhythmia, or irregular
heartbeat) is a group of conditions in which
the heartbeat is irregular, too fast, or too
slow.[2] A heart rate that is too fast – above
100 beats per minute in adults – is
called tachycardia and a heart rate that is too
slow – below 60 beats per minute – is
called bradycardia](https://image.slidesharecdn.com/cardiovascularsystem-180911082856/85/Cardiovascular-system-35-320.jpg)
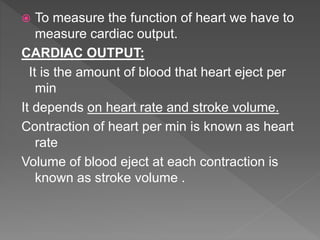
![ Ischemia or ischaemia is a restriction
in blood supply to tissues, causing a shortage
of oxygen that is needed for cellular metabolism (to
keep tissue alive).
[3]
Ischemia is generally caused by problems
with blood vessels, with resultant damage to or
dysfunction of tissue. It also means local anemia in
a given part of a body.
Ischemia comprises not only insufficiency of
oxygen, but also reduced availability
of nutrients and inadequate removal of metabolic
wastes. Ischemia can be partial (poor perfusion) or
total.](https://image.slidesharecdn.com/cardiovascularsystem-180911082856/85/Cardiovascular-system-36-320.jpg)


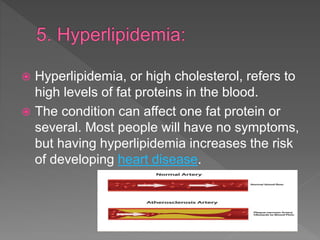


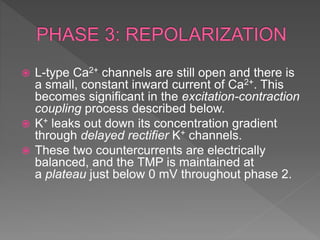
The cardiovascular system consists of the heart and blood vessels. The heart pumps blood through the vessels to supply all body tissues with oxygen and nutrients. It does this through the cardiac cycle of heart contraction and relaxation. The cardiac output, determined by heart rate and stroke volume, affects how much blood is pumped. Several factors influence stroke volume like preload, contractility, and afterload. Diseases that can affect the cardiovascular system include hypertension, arrhythmias, ischemia, heart failure, hyperlipidemia, and strokes.











































































