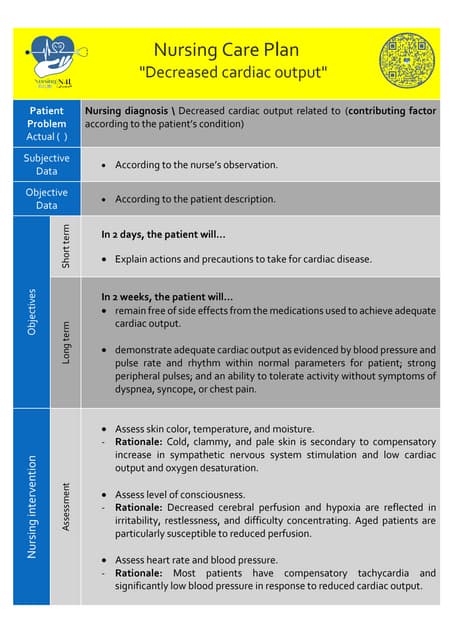
This document provides a nursing care plan for patients with congestive heart failure. It outlines several nursing diagnoses such as decreased cardiac output and impaired gas exchange. For each diagnosis, it lists goals and interventions. Interventions include placing the patient at rest, monitoring for signs of worsening heart failure, administering diuretics and monitoring fluid balance, gradually increasing activity, and providing patient education on managing their condition. The overall aim is to reduce the workload of the heart and improve oxygen delivery through non-pharmacological and pharmacological means.