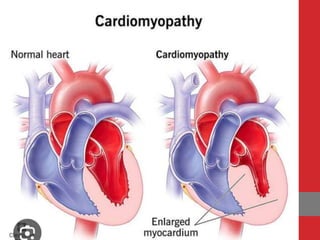
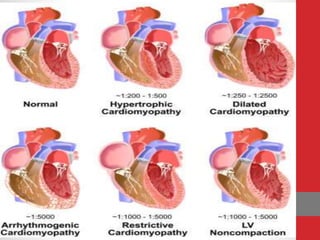
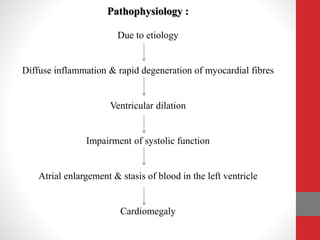
Cardiomyopathy is a disease of the heart muscle that affects its structure and ability to pump blood effectively. There are several classifications of cardiomyopathy including dilated, hypertrophic, restrictive, arrhythmogenic right ventricular, and unclassified. The document discusses the definitions, incidence, classifications, etiologies, pathophysiology, clinical features, diagnostic studies, and management of the different types of cardiomyopathy.