Downloaded 85 times
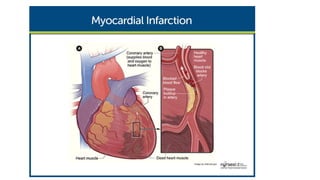
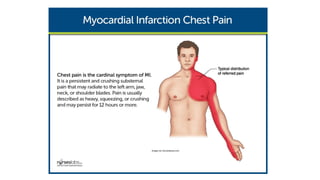




The document discusses myocardial infarction (MI), including its definition, classification, diagnosis, prevention, management in acute and long-term settings, nursing perspectives, and assessment. MI, also known as a heart attack, is caused by the death of heart muscle due to inadequate blood flow. Treatment aims to reopen blocked arteries, reduce clot size, lower risk of further issues, and prevent future MIs through medications, procedures like angioplasty, lifestyle changes, and ongoing management of conditions like high blood pressure and high cholesterol.

![MYOCARDIAL INFARCTION [presentation ]](https://cdn.slidesharecdn.com/ss_thumbnails/mipresentationnew-200825060434-thumbnail.jpg?width=640&height=640&fit=bounds)














































































