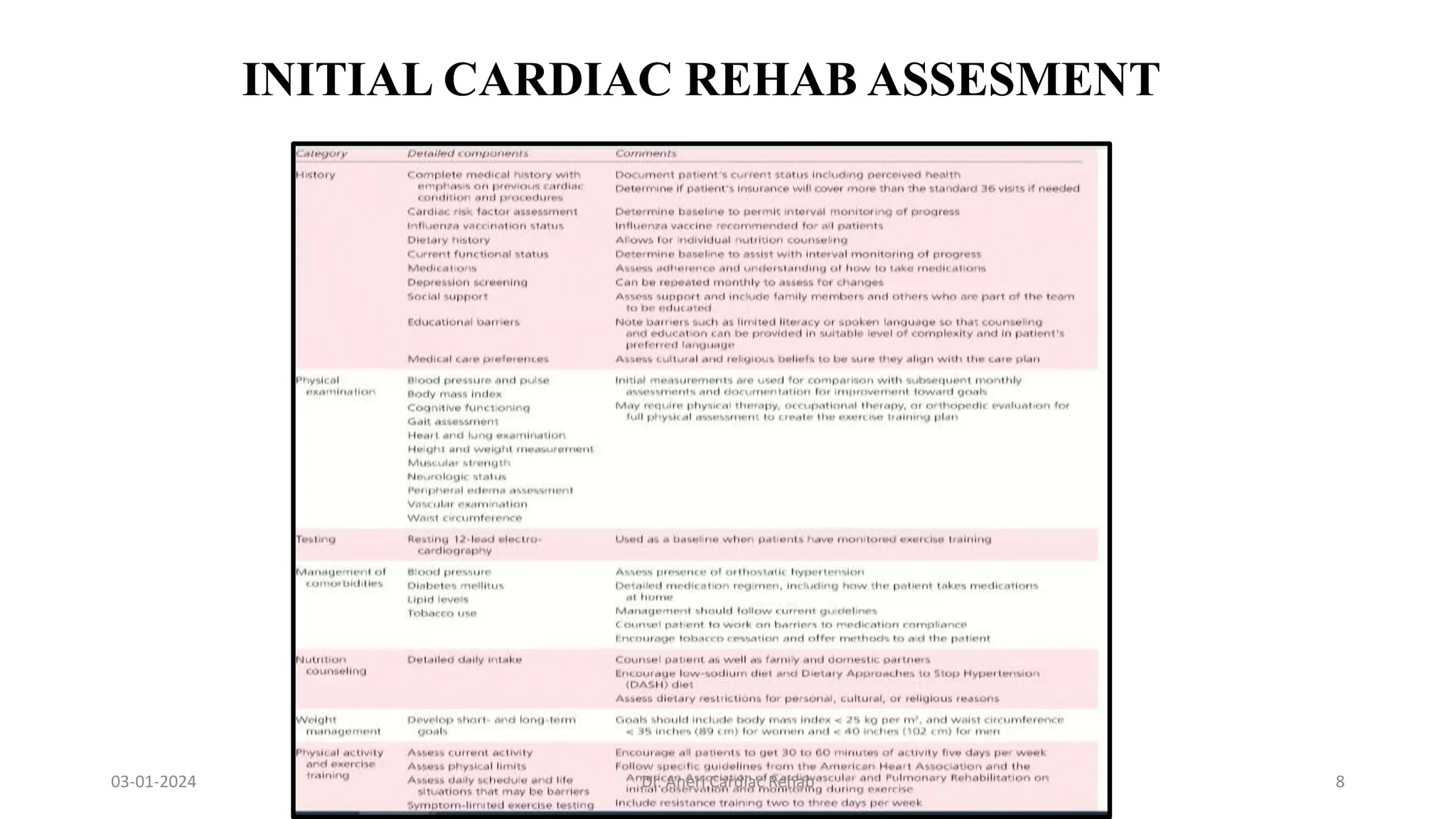
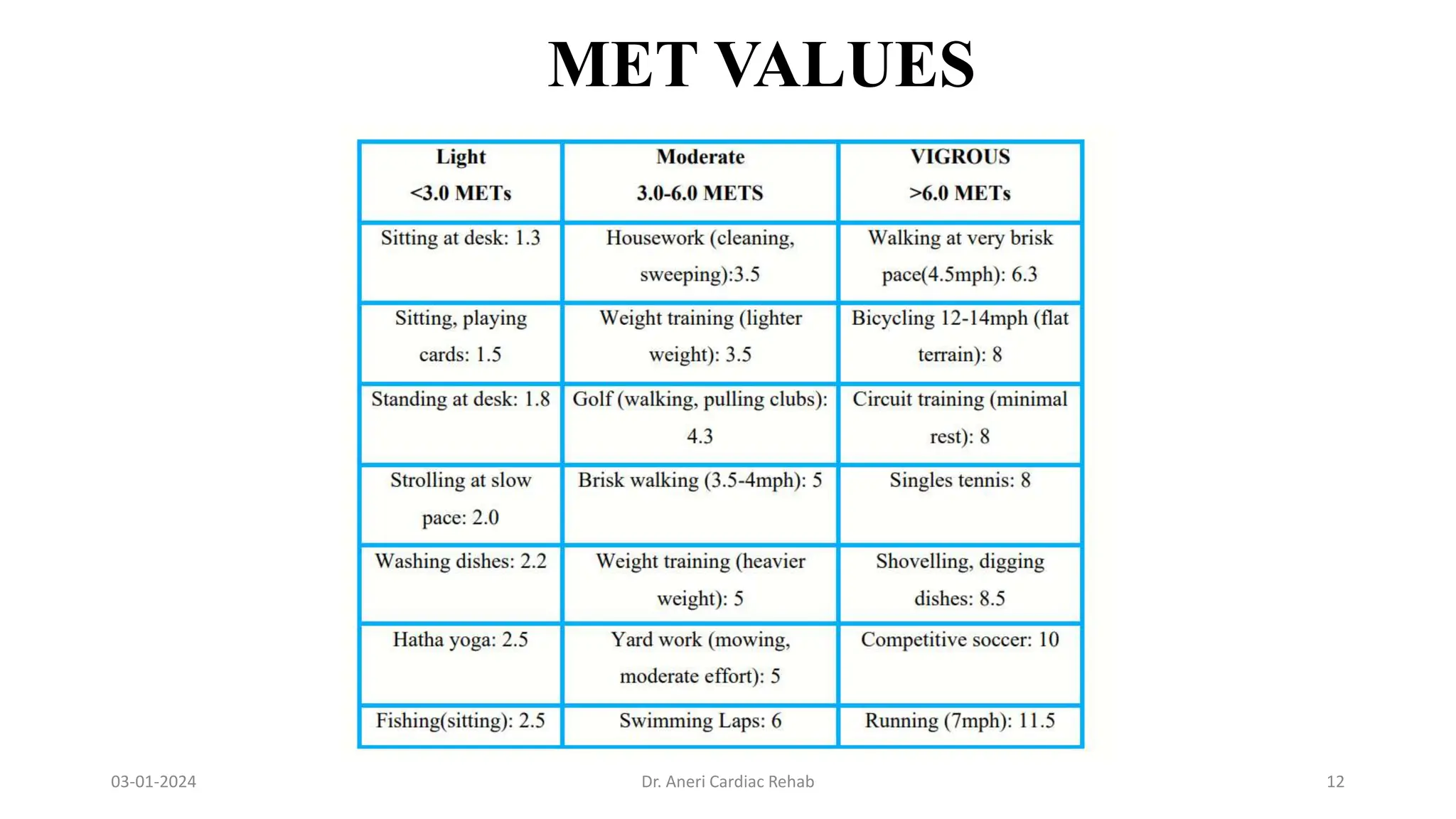
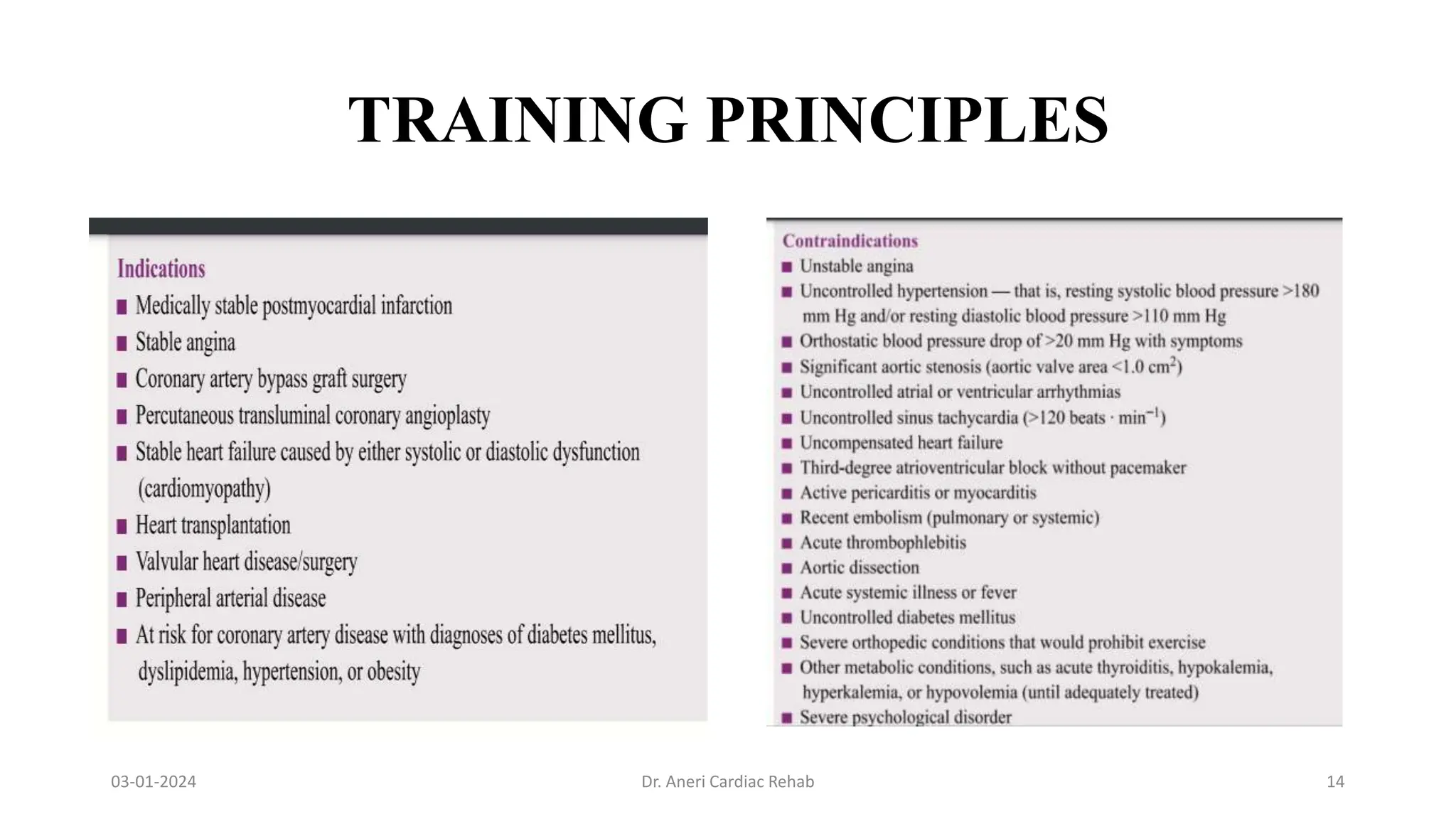
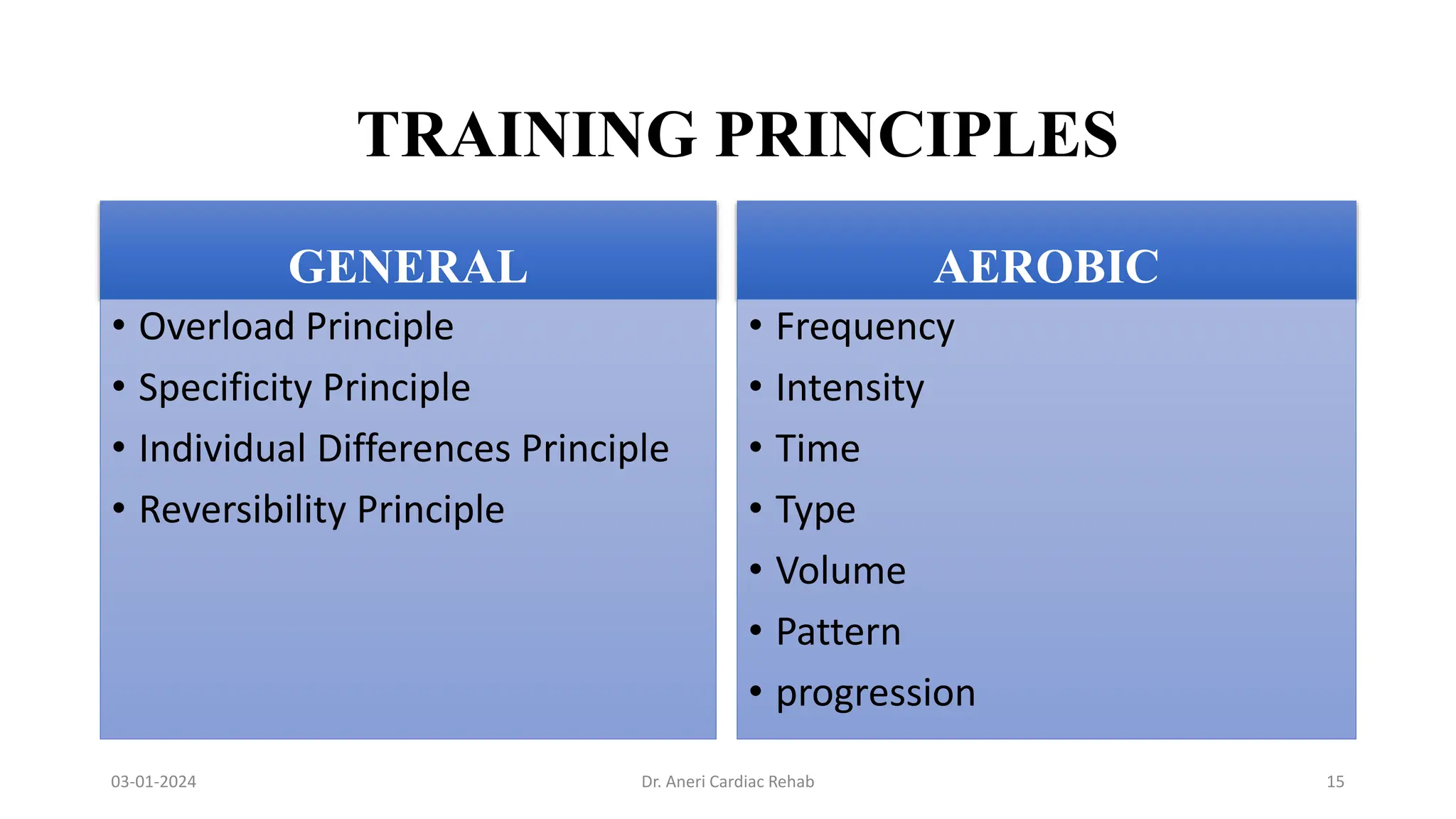
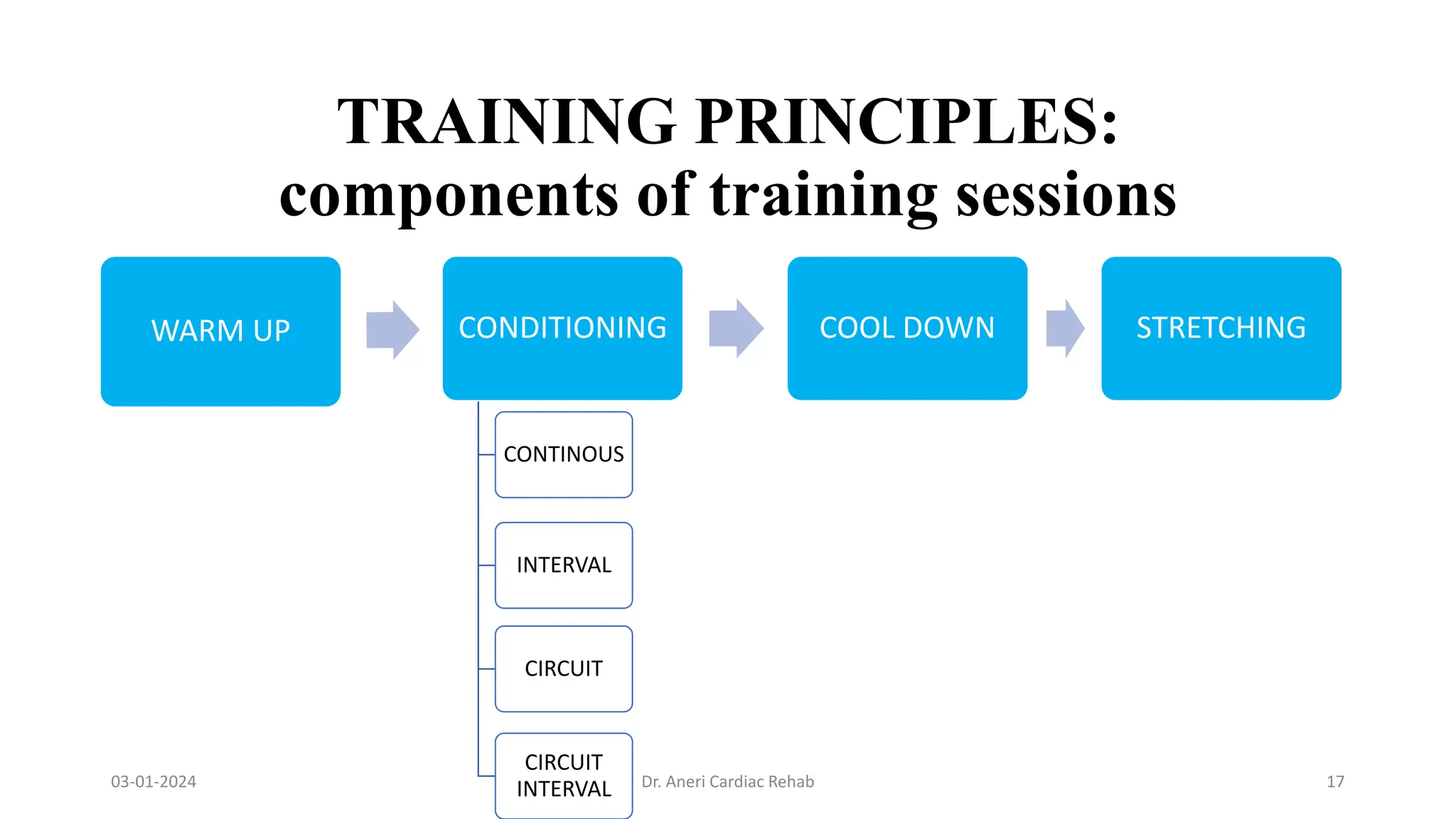
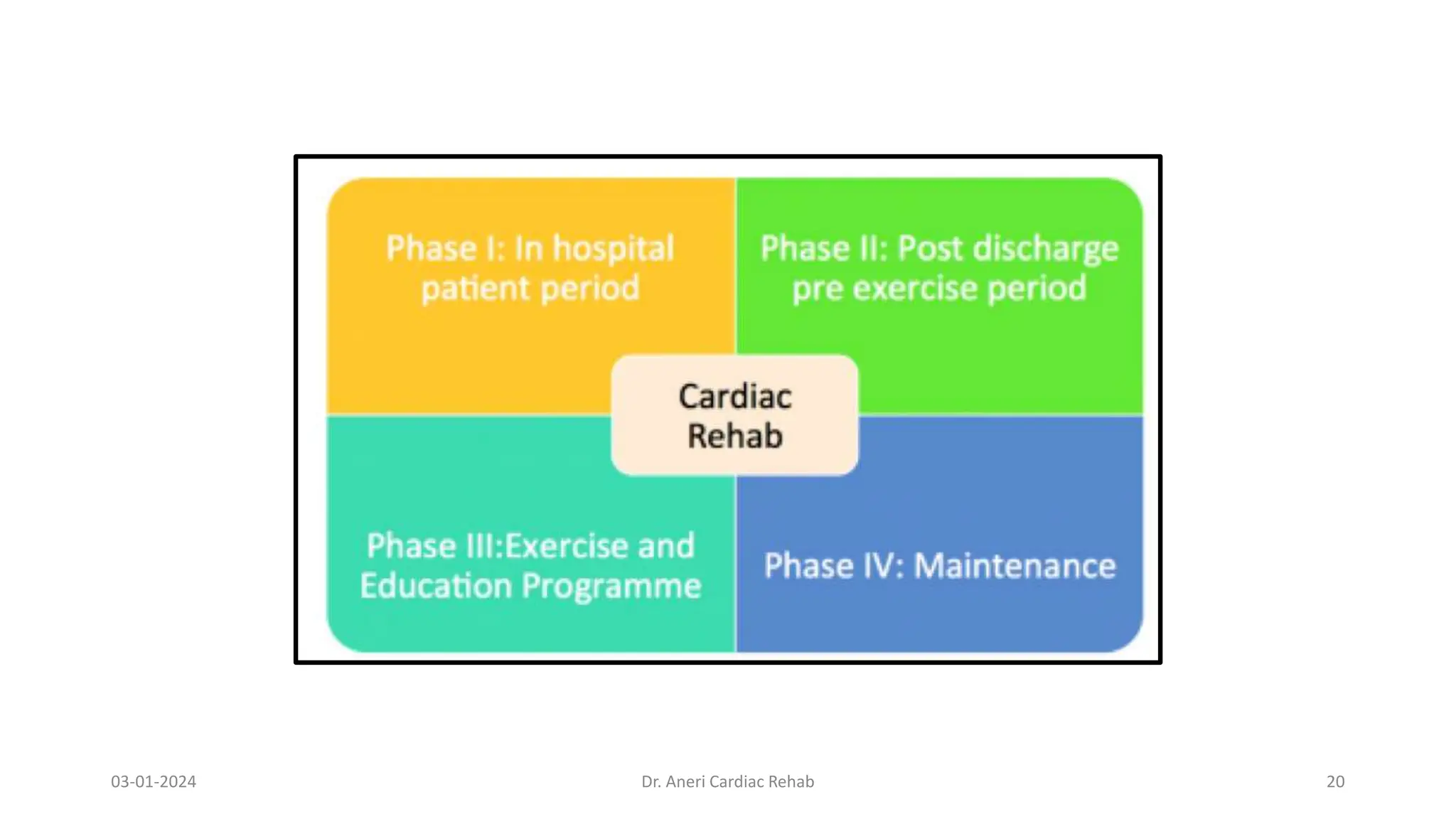
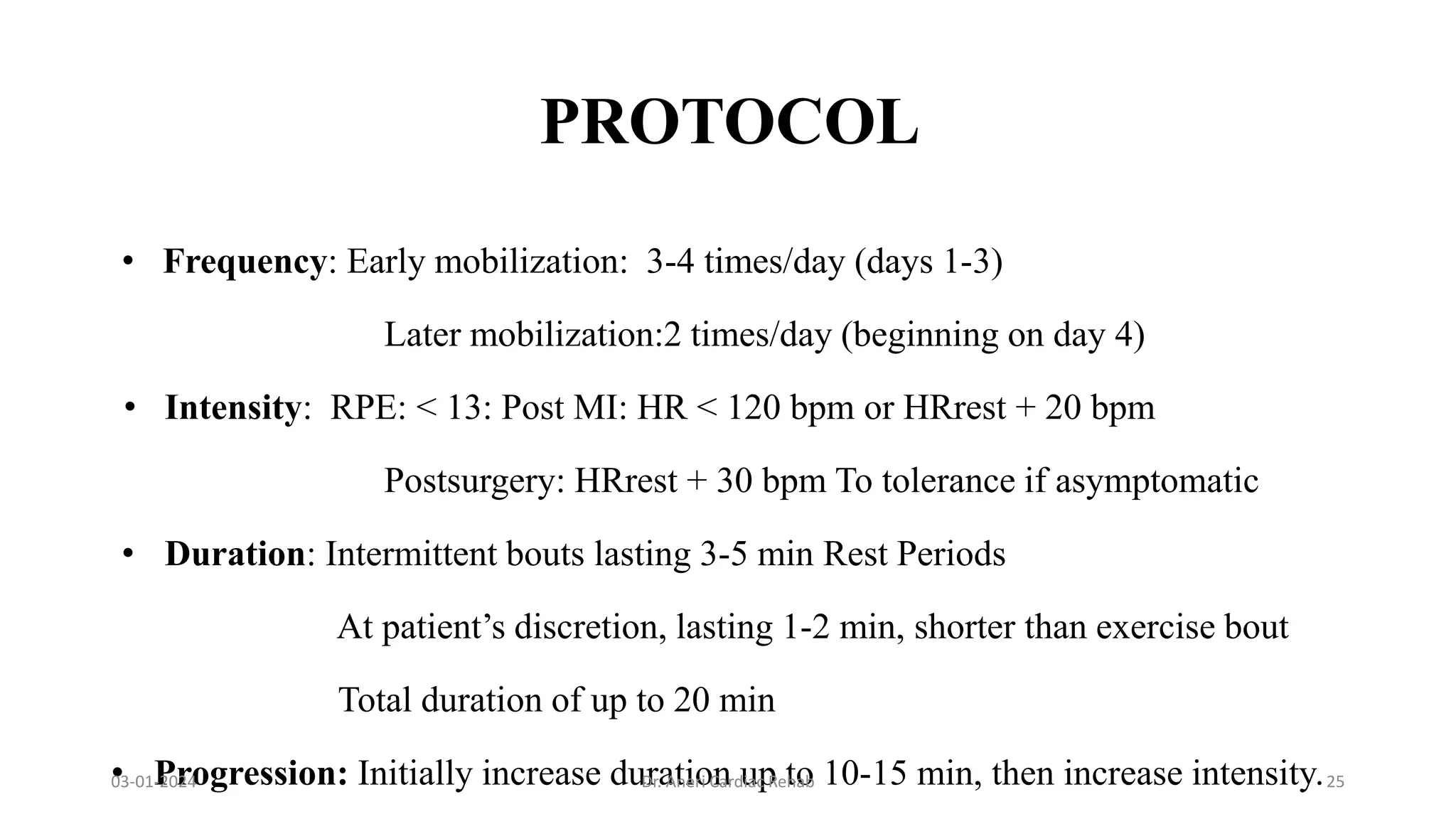
Cardiac rehabilitation is a multidisciplinary program aimed at educating and assisting individuals with heart disease to improve their physical and psychological health. Core components include assessment, structured physical activity, risk factor reduction, and psychological support. The rehabilitation process is divided into phases with specific exercises and training principles tailored to each patient's needs.