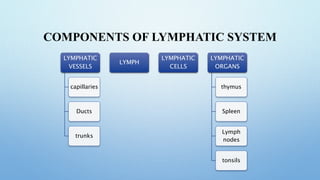
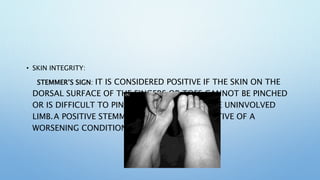
Lymphoedema is characterized by the excessive accumulation of fluid and proteins in tissues due to lymphatic system dysfunction, commonly presenting in the extremities with symptoms like heaviness, pain, and mobility limitations. It can be primary or secondary, and its management includes Complete Decongestive Therapy (CDT), which incorporates manual lymphatic drainage, compression therapy, exercise, and skin care. Effective self-management and education are critical for patients to minimize the risks of worsening lymphedema and associated complications.



![PHASES OF CDT
ACTIVE PHASE (PHASE 1)
• CONSISTS OF THE MOBILIZATION OF FLUID
AND THE INITIATION OF A DECREASE IN THE
PROLIFERATED CONNECTIVE TISSUE[1].
• THE NUMBER OF WEEKS DEPENDS ON THE
AMOUNT OF SWELLING AND TISSUE FIRMNESS.
• COMPLETE DECONGESTIVE THERAPY FOR
ONE-HOUR SESSIONS, 4 TO 5 DAYS PER WEEK.
• BANDAGES WITH FOAM ARE WORN ABOUT 23
HOURS PER DAY AND OFTEN ONLY REMOVED
TO BATHE.
MAINTENANCE PHASE (PHASE 2)
• MMAINTAINS THE SWELLING REDUCTION AND
AIMS FOR OPTIMIZATION OF CONNECTIVE
TISSUE REDUCTION
• SHOULD LAST FOR MONTHS OR FOR YEARS.
• ELASTIC COMPRESSION GARMENTS THAT FIT
LIKE A SECOND SKIN ARE WORN DURING THE
DAY.
• OFTEN BANDAGES WITH FOAM ARE WORN AT
NIGHT TO DECREASE DAILY DAYTIME
SWELLING.
• EXERCISES ARE DONE WHILE WEARING
COMPRESSION.
• SELF MANUAL LYMPHATIC DRAINAGE IS DONE
FOR 20 MINUTES PER DAY.](https://image.slidesharecdn.com/lymphoedema-240408041237-59aaffea/85/PHYSIOTHERAPY-IN-LYMPHOEDEMA-CONDITION-pptx-33-320.jpg)

![PHASE I WITH COMPRESSION
BANDAGES:
• BANDAGING IS A MAINSTAY OF TREATMENT
FOR STAGE 2 AND STAGE 3 LYMPHEDEMA
(MODERATE TO SEVERE LYMPHEDEMA).
• BANDAGING INVOLVES CREATING A SOFT CAST
ON THE ARM OR UPPER BODY BY WRAPPING
WITH MULTIPLE LAYERS.
• MAIN COMPONENT OF THECDT.
• BANDAGING IS A REDUCTIVE THERAPY,
MEANING IT MAKES THE LIMB SMALLER. WHEN
THE ARM IS BANDAGED, MUSCLES ARE “HELD
IN” BY THE MULTI-LAYER SOFT CAST EVERY
TIME THE ARM IS USED (THIS IS KNOWN AS
WORKING PRESSURE).
PHASE II WITH MEDICAL COMPRESSION GARMENTS:
• COMPRESSION GARMENTS ARE DESIGNED TO KEEP A CONTINUOUS
PRESSURE ON THE SWOLLEN/AFFECTED AREA TO ASSIST THE
DRAINAGE OF FLUID AND MINIMIZE SWELLING. IMAGE R:
LYMPHEDEMA COMPRESSION SLEEVE, DISPLAYED ON MANNEQUIN
• EXTERNAL COMPRESSION PROVIDES A COUNTER FORCE TO THE
WORKING MUSCULATURE (IE WORKING PRESSURE).
• WORKING PRESSURE HELPS TO PREVENT RE-ACCUMULATION OF
FLUIDS WHICH WERE EVACUATED DURING INTENSIVE COMPLETE
DECONGESTIVE THERAPY (CDT) AND CONSERVE THE RESULTS
ACHIEVED DURING MANUAL LYMPHATIC DRAINAGE (MLD)[4].
• SLEEVE WORN ON THE ARM, FINGERLESS GLOVE OR A GAUNTLET
(WHICH DOES NOT HAVE INDIVIDUAL FINGER OPENINGS), OFTEN
WORN WITH A SLEEVE
• ALL OF THE GARMENTS ARE MADE OF FLEXIBLE FABRIC. SLEEVES
ARE TIGHTER AT THE BOTTOM THAN THEY ARE AT THE TOP
CREATING THE GRADED PRESSURE THAT KEEPS THE LYMPH MOVING
OUT OF THE ARM. THERE IS A VARIETY OF FABRICS AVAILABLE: SOME
FEEL SOFTER, OTHERS STIFFER, AND SOME MAY INCLUDE MATERIALS
SUCH AS WOOL OR LATEX.
COMPRESSION THERAPY](https://image.slidesharecdn.com/lymphoedema-240408041237-59aaffea/85/PHYSIOTHERAPY-IN-LYMPHOEDEMA-CONDITION-pptx-39-320.jpg)



![SELF-CARE MANAGEMENT AND TRAINING
• Education regarding “self care” (ie everything client does at home to reduce the risk of the lymphedema coming back or getting worse in
the future) is vital. As a lymphedema therapist you should teach clients how to
• Put on and care for their compression sleeves and garments. Patients need to understand the need to replace the garments on a regular basis
to maintain sufficient compression. Each garment should be washed daily to restore the compression and replaced after 3 to 6 months of
continuous use, although very active patients may require these to be changed sooner[8].
• Protecting arm, hand, chest, or other body part from cuts, injury, overuse, extreme temperatures, and other situations that can increase the
production of lymph, which in turn increases lymphedema risk
• Educate re the signs and symptoms of infection, which is a special concern for people with lymphedema
• Help plan and set an individualised exercise and/or weight control plan
• Teach how to do manual lymphatic drainage on their own, at home. If “self-mld” is appropriate and client can manage technique. Stress to
client that doing more than is recommended, or being more aggressive with the massage strokes for MLD, could be harmfu](https://image.slidesharecdn.com/lymphoedema-240408041237-59aaffea/85/PHYSIOTHERAPY-IN-LYMPHOEDEMA-CONDITION-pptx-50-320.jpg)


















![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)































































