Downloaded 615 times

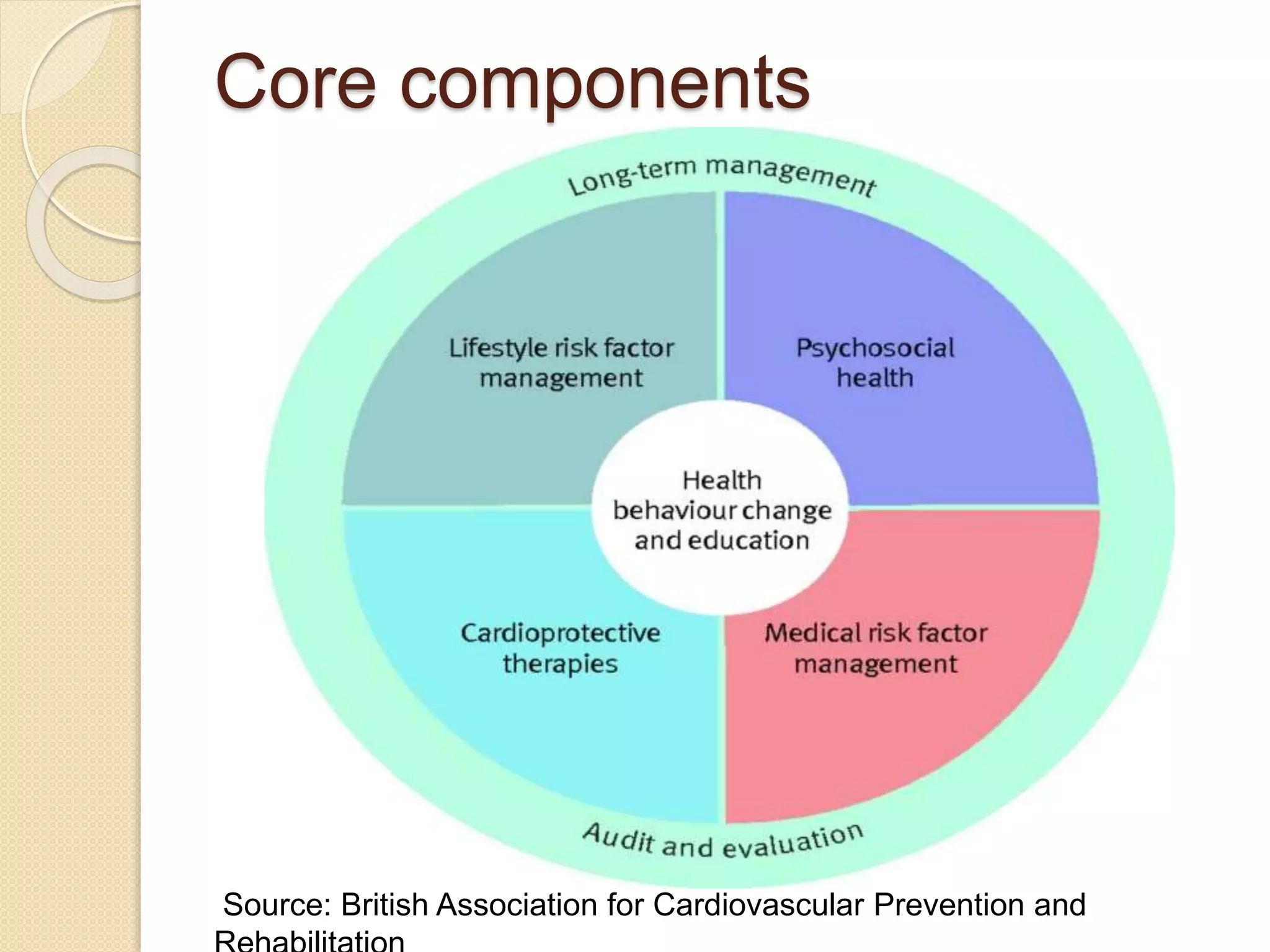




























































Cardiac rehabilitation aims to optimize physical, psychological, and social functioning for cardiac patients through coordinated interventions. It includes exercise training, risk factor management, and education. Rehabilitation occurs in phases: phase I in the hospital focuses on mobilization; phase II after discharge emphasizes education and gradual activity; phase III incorporates supervised exercise and ongoing support; and phase IV is long-term maintenance. The goals are to improve symptoms, quality of life, and prognosis through lifestyle changes and secondary prevention.





















































































