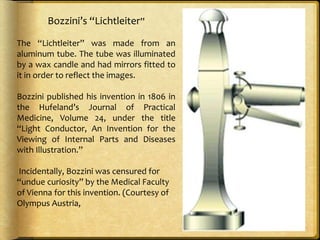
The document describes the history and development of endoscopy from its origins with Bozzini's "Lichtleiter" in 1806 to modern innovations. Key developments include:
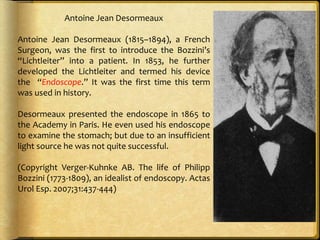
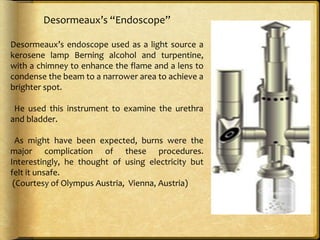
- Desormeaux introducing Bozzini's device into patients and coining the term "endoscope" in 1853.
- Czerny constructing the first rigid endoscope in 1880 and using Edison's light bulb, allowing angling and air insufflation.
- Kelling pioneering laparoscopy in 1901 after being introduced to endoscopy by Mikulicz-Radecki.
- Hopkins inventing the rigid rod-lens system for scopes in 1959, allowing their widespread adoption after partnering with










































































![Microscopes 1[1]/ orthodontic course by indian dental academy](https://cdn.slidesharecdn.com/ss_thumbnails/microscopes11-140427071202-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





















