The document discusses heart transplantation, including:
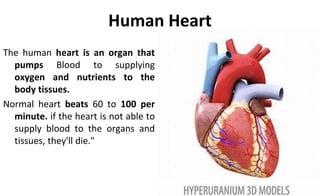
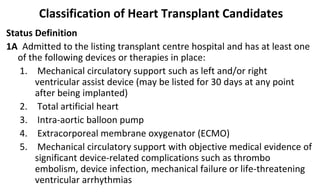
- The normal function of the human heart and what happens when it is not able to supply blood properly.
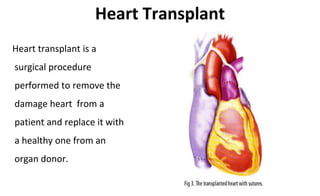
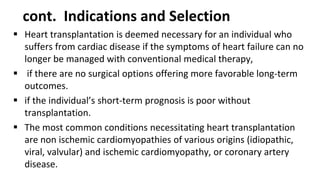
- That heart transplantation involves replacing a damaged heart with a healthy donor heart through surgery.
- Some details about the first successful heart transplant performed in India in 1994 and hospitals approved to perform the procedure.
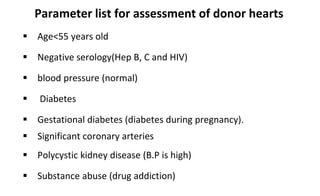
- Criteria for determining donor heart suitability and matching it to a recipient, including blood type and body size compatibility.
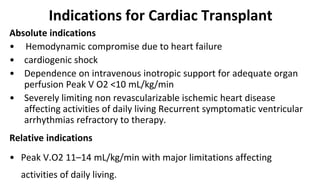
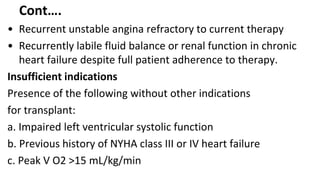
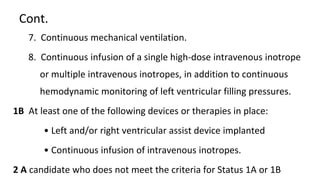
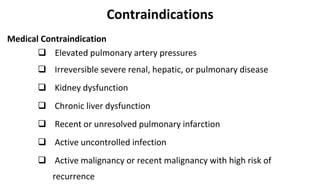
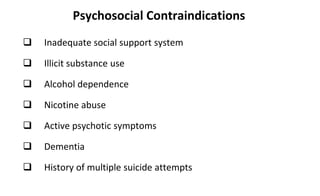
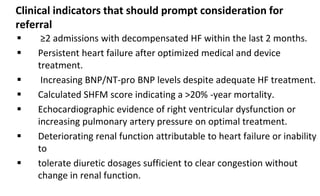
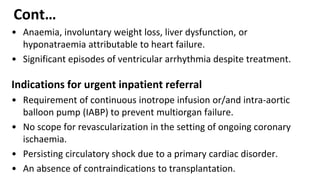
- Indications and contraindications for receiving a heart transplant.
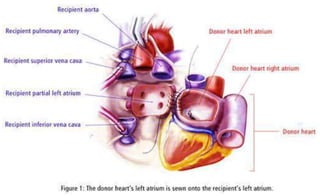
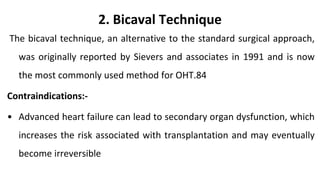
- Surgical techniques for transplantation, including the biatrial technique which is the standard orthotopic heart transplant procedure.


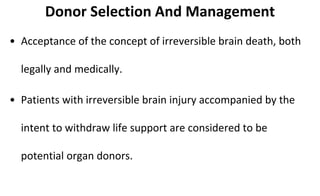
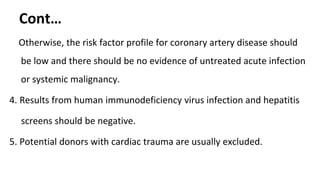
![Criteria For Determining Brain Death
Clinical Evaluation
• Mechanism of brain injury is sufficient to account for irreversible loss
of brain function
• Absence of reversible causes of CNS depression
• CNS depressant drugs
• Hypothermia (<32°C [85°F])
• Hypotension (MAP <55 mmHg)
• Absence of neuromuscular blocking drugs that may confound the
results of the neurologic exam
• No spontaneous movements, motor responses, or posturing](https://image.slidesharecdn.com/hearttyransplantation-190912083604/85/Heart-tyransplantation-9-320.jpg)



































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



