Downloaded 15 times

![ETIOLOGY
The exact cause is unknown .
A] Coitus and sperm factor .
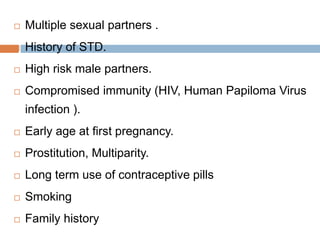
B] Risk factor for cervical .
1.Actual risk factor.
Low socio-economic status.
Early age of first coitus.](https://image.slidesharecdn.com/ca-cervix-201226071828/85/Ca-cervix-6-320.jpg)
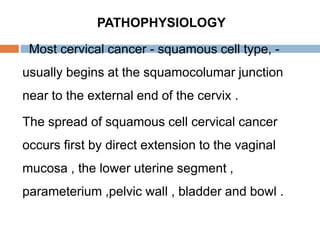
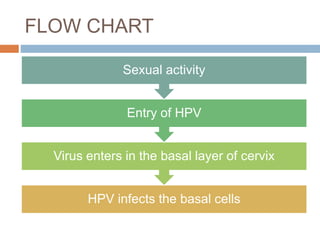

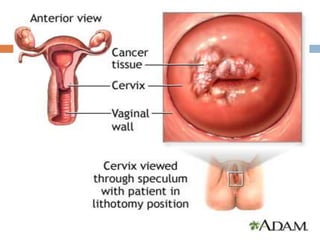
This document outlines the learning objectives related to cervical cancer (ca-cervix), covering its definition, etiology, pathophysiology, stages, clinical features, diagnostic evaluations, and management strategies. Cervical cancer is primarily a squamous cell carcinoma affecting women, with risk factors including socio-economic status, early sexual activity, and HPV infection. The management varies by stage and includes surgical options, radiotherapy, and nursing care to address patient concerns and promote recovery.























































































