Introduction
• “lazy eye”
•Form of cortical visual impairment
• Results from abnormal visual development in
childhood
• Secondary to another pathological process
• Can lead to permanent reduced vision
• It affects a variety of visual functions
5.
Definition
• condition withu/l or b/l subnormal vision
– at least two lines less than ‘normal’ or two lines
less than the fellow eye in unilateral cases
• without any local ophthalmoscopic
abnormality
• which is reversible if treated appropriately at
the proper time
6.
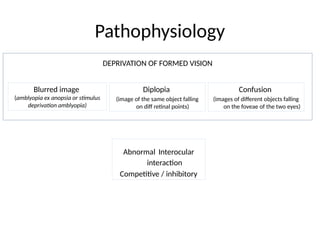
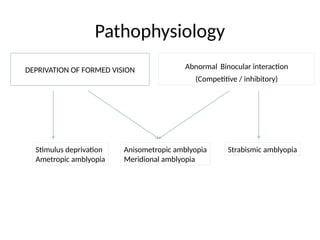
Pathophysiology
Blurred image
(amblyopia exanopsia or stimulus
deprivation amblyopia)
Diplopia
(image of the same object falling
on diff retinal points)
Confusion
(images of different objects falling
on the foveae of the two eyes)
Abnormal Interocular
interaction
Competitive / inhibitory
DEPRIVATION OF FORMED VISION
7.
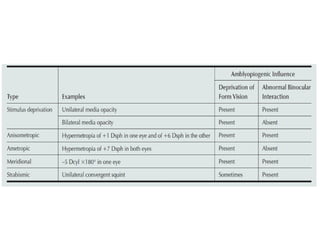
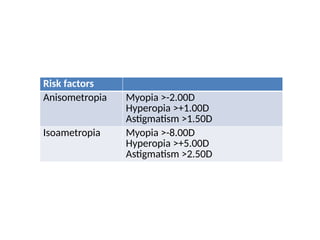
Classification: by cause
•Strabismic
• Refractive
– Anisometropia
– High bilateral refractive (isoametropic)
• Visual stimulus deprivation (Amblyopia ex anopsia) (B/L
or U/L)
– Media opacities
– Ptosis
• Occlusion (reverse)
• Nystagmus related
Strabismic amblyopia
• Mostcommon form of amblyopia
• Constant
• Nonalternating
• Unequally alternating tropias (typically
esodeviations)
11.
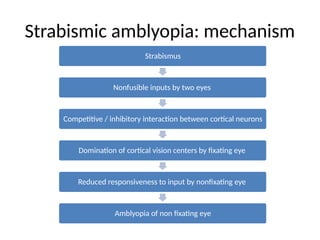
Strabismus
Nonfusible inputs bytwo eyes
Competitive / inhibitory interaction between cortical neurons
Domination of cortical vision centers by fixating eye
Reduced responsiveness to input by nonfixating eye
Amblyopia of non fixating eye
Strabismic amblyopia: mechanism
12.
Refractive Amblyopia
• D/Tuntreated unilateral or bilateral refractive errors
• Anisometropic amblyopia
– Unilateral amblyopia
– Cause
• Blurred image in one eye
• Interocular Competitive / inhibitory interaction
– Greater degrees of anisometropia or astigmatism (meridional) result in
increased risk and severity of amblyopia
– May occur in combination with strabismus
• Bilateral refractive amblyopia (isoametropic)
– less common form of refractive amblyopia
– bilateral reduction in visual acuity
– Cause- blurred retinal images alone
– More common in children with hypermetropia of >5 D
– Less common with high myopia as the near vision is intact
Visual Deprivation Amblyopia
•Caused by complete or partial obstruction of visual axis degraded
retinal image
• Least common form of amblyopia
• Causes
– Congenital or early-onset cataract (MC)
– Corneal opacities
– Intraocular inflammation
– Vitreous hemorrhage
– Ptosis
• Most severe and difficult to treat
• Visual loss is more as comp to bilateral deprivation of similar degree
interocular competition adds to the direct amblyogenic impact of
severe image degradation
15.
Visual Deprivation Amblyopia:Cataract
• In Newborns good prognosis if removed and optical
correction is in place by 2 months of age
• Bilaterally symmetrical cataract the interval between
the surgery for the two eyes should be one to two
weeks at the maximum
• < 6 years of age dense central cataracts cause
amblyopia
• > 6 years less amblyogenic
• Polar and lamellar cataracts cause mild to moderate or
no amblyopia
16.
Occlusion (Reverse Amblyopia)
•Specific form of deprivation amblyopia
• Seen after therapeutic patching or cycloplegia
of the nonamblyopic eye
• Visual acuity returns to baseline with no active
therapy discontinuation of the current
therapy
• Lower doses of patching and atropinelower
rates of reverse amblyopia
17.
Natural History
• Lifelongvisual loss if untreated or inadequately treated in early childhood
• Successful treatment greatest in young children
• Older children CAN improve visual acuity
• Deprivation amblyopia
• First 3 postnatal mths profound and permanent reductions in acuity (20/200 or
worse)
– Strong association with sensory nystagmus in b/l cases and strabismus in both u/l
and b/l cases
• After 3 months of age less profound visual acuity reduction
– Deprivation at later ages shows a slower rate of vision loss, and the child is more
likely to respond to treatment
• Untreated refractive or strabismic amblyopia- less severe visual acuity deficits
• Risk of amblyopia is reduced with age
• Amblyopia is risk factor
– Strabismus
– Subnormal binocularity. In young children, amblyopia treatment may improve vision
and may foster the development of binocular vision
18.
Diagnosis: History
• Thechief complaint
• Current eye problems
• Ocular history, including prior eye problems, diseases, diagnoses, and
treatments
• Systemic history
– Gestational age of less than 30 weeks
– Birth weight less than 1500 grams
– Prenatal and perinatal history (e.g., alcohol, tobacco, and drug use during
pregnancy)
– Past hospitalizations and operations
– General health and development including developmental delay or cerebral palsy
• Current medications and allergies
• Family history of ocular conditions and relevant systemic conditions
19.
Diagnosis: Examination
• Comprehensiveophthalmic evaluation
• Attention to risk factors for amblyopia
– Strabismus
– Anisometropia
– Media opacity or structural defects
– Uveitis
– Ptosis
– Delayed visual or neurologic maturation of unclear etiology
– Cerebral palsy
– Syndromes with ocular involvements such as Down syndrome
– Family history of amblyopia, strabismus, childhood cataract, or
childhood glaucoma
20.
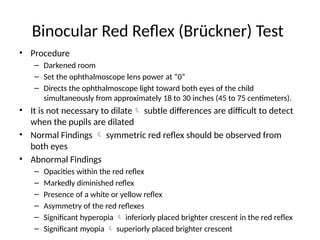
Binocular Red Reflex(Brückner) Test
• Procedure
– Darkened room
– Set the ophthalmoscope lens power at “0”
– Directs the ophthalmoscope light toward both eyes of the child
simultaneously from approximately 18 to 30 inches (45 to 75 centimeters).
• It is not necessary to dilate subtle differences are difficult to detect
when the pupils are dilated
• Normal Findings symmetric red reflex should be observed from
both eyes
• Abnormal Findings
– Opacities within the red reflex
– Markedly diminished reflex
– Presence of a white or yellow reflex
– Asymmetry of the red reflexes
– Significant hyperopia inferiorly placed brighter crescent in the red reflex
– Significant myopia superiorly placed brighter crescent
21.
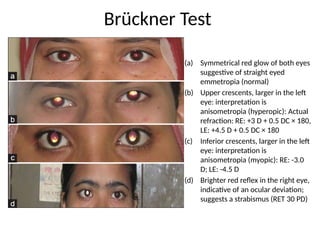
(a) Symmetrical redglow of both eyes
suggestive of straight eyed
emmetropia (normal)
(b) Upper crescents, larger in the left
eye: interpretation is
anisometropia (hyperopic): Actual
refraction: RE: +3 D + 0.5 DC × 180,
LE: +4.5 D + 0.5 DC × 180
(c) Inferior crescents, larger in the left
eye: interpretation is
anisometropia (myopic): RE: -3.0
D; LE: -4.5 D
(d) Brighter red reflex in the right eye,
indicative of an ocular deviation;
suggests a strabismus (RET 30 PD)
Brückner Test
22.
Visual Acuity inAmblyopia
Specific characteristics of amblyopic visual acuity
• Crowding phenomenon- Single letter vision is better than if
the letters are presented in a row as in visual acuity charts
• Visual acuity drops less when viewed through grey neutral-
density filters compared to normal eyes
• Decreased contrast sensitivity and spatial localization
• Impaired pursuit eye movements
• Decreased saccadic amplitudes
• Grating visual acuity is less affected than the resolution
visual acuity for letters
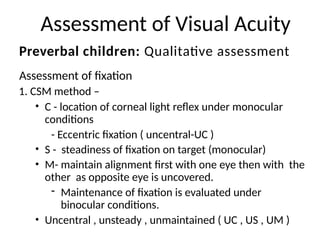
Assessment of VisualAcuity
Assessment of fixation
1. CSM method –
• C - location of corneal light reflex under monocular
conditions
- Eccentric fixation ( uncentral-UC )
• S - steadiness of fixation on target (monocular)
• M- maintain alignment first with one eye then with the
other as opposite eye is uncovered.
- Maintenance of fixation is evaluated under
binocular conditions.
• Uncentral , unsteady , unmaintained ( UC , US , UM )
Preverbal children: Qualitative assessment
25.
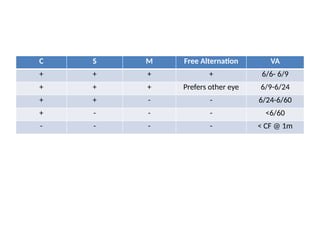
C S MFree Alternation VA
+ + + + 6/6- 6/9
+ + + Prefers other eye 6/9-6/24
+ + - - 6/24-6/60
+ - - - <6/60
- - - - < CF @ 1m
26.
Assessment of FixationPattern
Types of fixation
• Central fixation ( foveolar )
• Eccentric fixation ( non- foveolar )
– para-foveal within 2° of the fovea.
• No fixation ( erratic )- no definite area of fixation
around the true fovea
– Paramacular :- b/w 2° to 4° away from true fovea.
– Centrocaecal :- > 4° b/w the macula & optic disc.
– Paracaecal :- around optic disc.
27.
2. F andF method- Fixation and Following
– Procedure- drawing the child’s attention to the examiner
or caregiver’s face or to a hand-held light, toy, or other
fixation target and then slowly moving the target.
– Normal behavior recorded as “fixes and follows”
– Fixation preference assessed by observing the vigor
with which the child objects to occlusion of one eye
relative to the other
– Children resist covering an eye when the fellow eye has
limited vision
28.
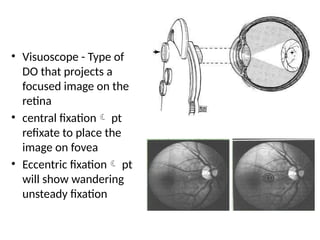
• Visuoscope -Type of
DO that projects a
focused image on the
retina
• central fixation pt
refixate to place the
image on fovea
• Eccentric fixation pt
will show wandering
unsteady fixation
29.
• Qualitative assessmentof visual acuity should
be replaced with a recognition visual acuity
test based on optotypes (letters, numbers, or
symbols) as soon as the child can perform this
task reliably
30.
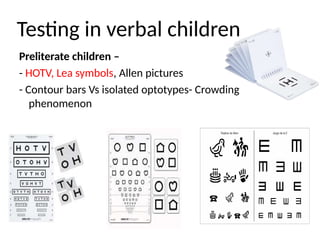
Testing in verbalchildren
Preliterate children –
- HOTV, Lea symbols, Allen pictures
- Contour bars Vs isolated optotypes- Crowding
phenomenon
31.
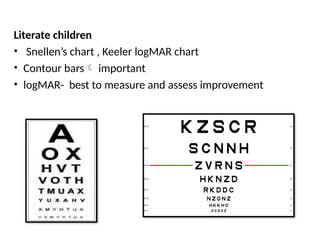
Literate children
• Snellen’schart , Keeler logMAR chart
• Contour bars important
• logMAR- best to measure and assess improvement
32.
Binocular Alignment andOcular
Motility
• Binocular Alignment
– Corneal light reflection
– Binocular red reflex (Brückner) test
– Cover tests
– Cover/uncover tests for tropias
– Alternate cover tests for the total deviation (latent
component included) in primary gaze at distance and near
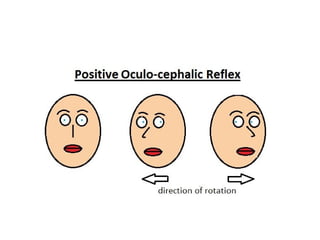
• Motility
– Ocular versions and ductions should be tested
– Eye movements may be tested using oculocephalic rotation
(doll’s head maneuver)
– Observing spontaneous eye movements in the inattentive or
uncooperative child.
34.
• Cycloplegic Retinoscopy/Refraction
–Cycloplegic refraction subjective refinement of
Refractive error is important
• Anterior segment evaluation:
– Cataract or corneal scar
• Fundus examination:
– Any posterior segment pathology might be the
cause of decreased vision, so it has to be ruled out
by a proper posterior segment evaluation.
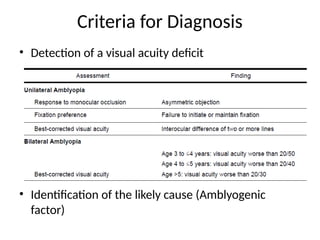
Criteria for Diagnosis
•Detection of a visual acuity deficit
• Identification of the likely cause (Amblyogenic
factor)
37.
PROGNOSIS
• Sensory deprivationamblyopia has a poorer
prognosis for rehabilitation than other forms of
amblyopia
• The earlier the therapy for amblyopia
management is started, the better is the
prognosis
• Hypermetropic anisometropic amblyopia has
worse prognosis than myopic anisometropic
amblyopia
38.
Management
• Success oftt declines with increasing age
• An attempt at treatment should be offered to
children regardless of age, including older
children and teenagers
• Strategies
– Firstcorrect the cause of visual deprivation
– Second correct refractive errors
– Third promote use of the amblyopic eye
• Goal equal visual acuity between the two eyes
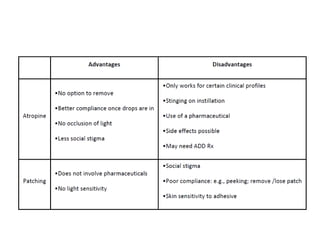
Occlusion types
• Lighttransmission
– Total
– Partial
• Duration
– Full time
– Part time
• Eye
– Conventional
– Inverse
42.
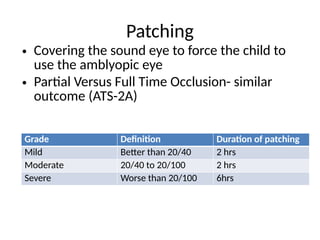
Patching
Grade Definition Durationof patching
Mild Better than 20/40 2 hrs
Moderate 20/40 to 20/100 2 hrs
Severe Worse than 20/100 6hrs
• Covering the sound eye to force the child to
use the amblyopic eye
• Partial Versus Full Time Occlusion- similar
outcome (ATS-2A)
Pharmacological treatment
• Cycloplegiaof the nonamblyopic eye
• Cycloplegia optically defocuses the nonamblyopic eye
• Treatment for children who do not improve with
eyeglasses alone
• Works best when the nonamblyopic eye is hyperopic
• May be considered in the presence of latent
nystagmus, occlusion failure, or for maintenance
treatment
• Drug used – Atropine 1%
Optical Treatment
• Alteringthe refractive correction of the fellow
eye typically blurring at distance by adding
1.00 to 3.00 diopters of plus sphere
• Encourage the amblyopic eye to take fixation
48.
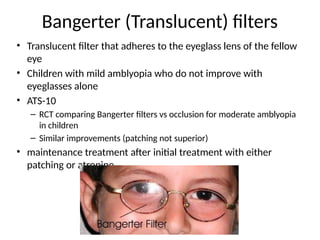
Bangerter (Translucent) filters
•Translucent filter that adheres to the eyeglass lens of the fellow
eye
• Children with mild amblyopia who do not improve with
eyeglasses alone
• ATS-10
– RCT comparing Bangerter filters vs occlusion for moderate amblyopia
in children
– Similar improvements (patching not superior)
• maintenance treatment after initial treatment with either
patching or atropine
49.
Surgery
• Indications
– Cataract
–Nonclearing vitreous Hge Vitrectomy
– Corneal opacities
– Blepharoptosis
– Refractive surgery in treating anisometropic
amblyopia is controversial
52.
Alternative Therapies
• Visiontherapy
– Aka “orthoptics,” or eye exercises
– nonsurgical program of visual activities to improve visual acuity
and binocularity
– computer programs, prisms, filters, vergence activities,
accommodation activities and eye-hand coordination exercises
• Binocular therapy
– Amblyopia with no strabismus or small-angle strabismus with
some binocularity
– Images are presented dichoptically high-contrast images are
presented to the amblyopic eye and low-contrast images are
presented to the fellow eye
54.
Alternative Therapies
• Pleoptics
–Bangerter coined the term ‘pleoptics’
– Principle in c/o eccentric fixation dazzle the eccentrically fixing
retinal area while protecting the fovea followed by direct
stimulation of the macula with flashes of light under observation
• CAM Stimulator
– Principle- active stimulation of the amblyopic eye to improve
vision in that eye
– High contrast spinning disk with square wave grating presented to
the amblyopic eye and better eye is covered
– Stimulates the amblyopic eye
– Daily for 10 to 14 minutes
55.
Alternative Therapies
• PharmacologicTherapy
– Levodopa is a precursor of dopamine, a neuromodulator
– works by increasing the levels of dopamine in the central nervous
system
– Levodopa-carbidopa found to have short term improvement in visual
acuity in amblyopes with recurrence of amblyopia
– The addition of occlusion therapy to levodopa-carbidopa leads to
sustained improvement in visual acuity
• Acupuncture
– Few studies mentioned acupuncture to be a modality to cure
amblyopia
– Acupuncture is applied with the use of auricular stickings
– Experimental
56.
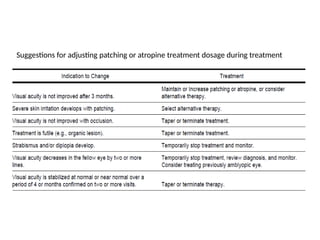
Follow-up Evaluation
• Purpose-monitor the response to therapy and
adjust the treatment plan as necessary
• Goal
– Determining the visual acuity of the amblyopic eye
– Interval history
• Adherence to the treatment plan
• Side effects of the treatment
– Visual acuity in the fellow eye
57.
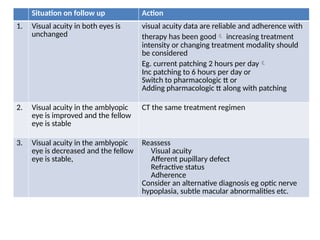
Situation on followup Action
1. Visual acuity in both eyes is
unchanged
visual acuity data are reliable and adherence with
therapy has been good increasing treatment
intensity or changing treatment modality should
be considered
Eg. current patching 2 hours per day
Inc patching to 6 hours per day or
Switch to pharmacologic tt or
Adding pharmacologic tt along with patching
2. Visual acuity in the amblyopic
eye is improved and the fellow
eye is stable
CT the same treatment regimen
3. Visual acuity in the amblyopic
eye is decreased and the fellow
eye is stable,
Reassess
Visual acuity
Afferent pupillary defect
Refractive status
Adherence
Consider an alternative diagnosis eg optic nerve
hypoplasia, subtle macular abnormalities etc.
58.
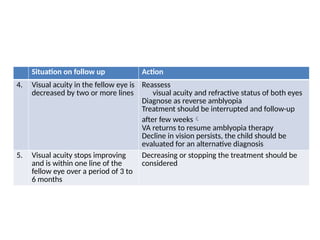
Situation on followup Action
4. Visual acuity in the fellow eye is
decreased by two or more lines
Reassess
visual acuity and refractive status of both eyes
Diagnose as reverse amblyopia
Treatment should be interrupted and follow-up
after few weeks
VA returns to resume amblyopia therapy
Decline in vision persists, the child should be
evaluated for an alternative diagnosis
5. Visual acuity stops improving
and is within one line of the
fellow eye over a period of 3 to
6 months
Decreasing or stopping the treatment should be
considered
59.
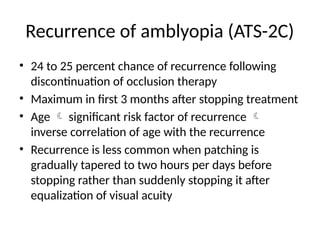
Recurrence of amblyopia(ATS-2C)
• 24 to 25 percent chance of recurrence following
discontinuation of occlusion therapy
• Maximum in first 3 months after stopping treatment
• Age significant risk factor of recurrence
inverse correlation of age with the recurrence
• Recurrence is less common when patching is
gradually tapered to two hours per days before
stopping rather than suddenly stopping it after
equalization of visual acuity
60.
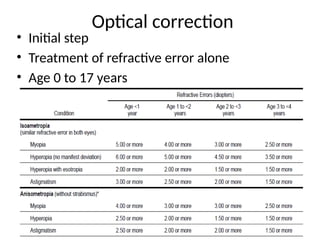
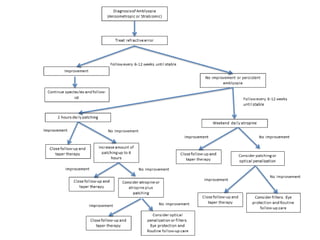
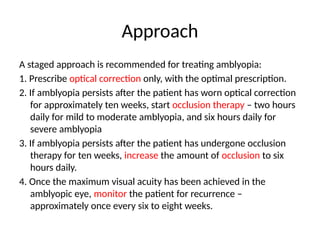
Approach
A staged approachis recommended for treating amblyopia:
1. Prescribe optical correction only, with the optimal prescription.
2. If amblyopia persists after the patient has worn optical correction
for approximately ten weeks, start occlusion therapy – two hours
daily for mild to moderate amblyopia, and six hours daily for
severe amblyopia
3. If amblyopia persists after the patient has undergone occlusion
therapy for ten weeks, increase the amount of occlusion to six
hours daily.
4. Once the maximum visual acuity has been achieved in the
amblyopic eye, monitor the patient for recurrence –
approximately once every six to eight weeks.
61.
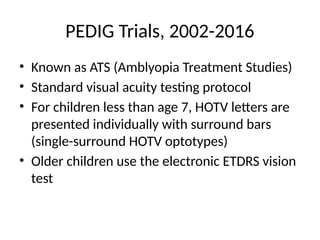
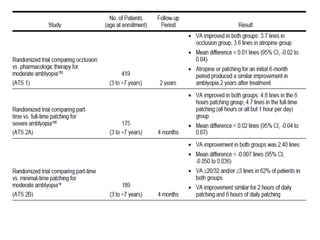
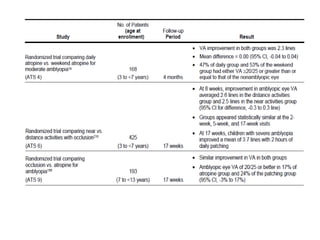
PEDIG Trials, 2002-2016
•Known as ATS (Amblyopia Treatment Studies)
• Standard visual acuity testing protocol
• For children less than age 7, HOTV letters are
presented individually with surround bars
(single-surround HOTV optotypes)
• Older children use the electronic ETDRS vision
test