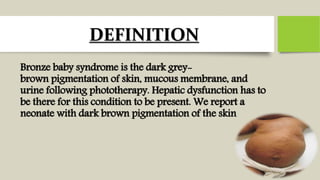
Bronze baby syndrome is a rare condition seen in premature infants undergoing phototherapy for jaundice. It causes intense grey-brown discoloration of the skin, serum, and urine. It is thought to be caused by pre-existing liver dysfunction preventing excretion of photooxidation products of bilirubin, leading to their deposition and discoloration. Risk factors include prematurity, undernutrition, reduced liver or kidney function, and high-dose chloramphenicol use. Management involves stopping phototherapy and supportive care; more severe cases may require exchange transfusion or dialysis.