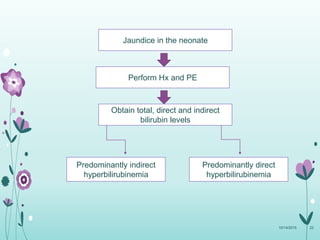
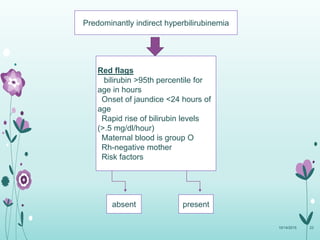
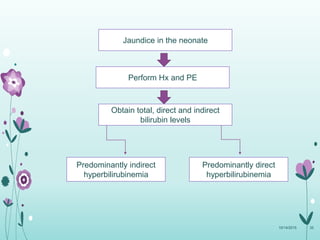
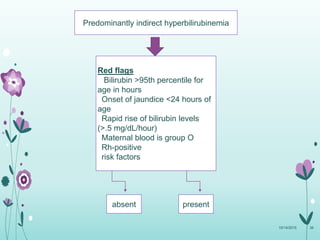
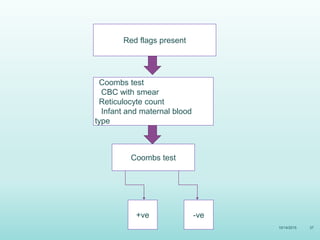
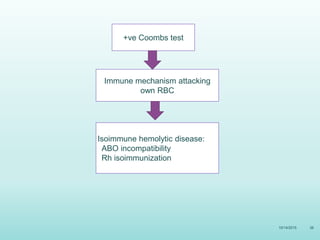
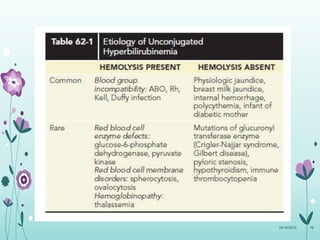
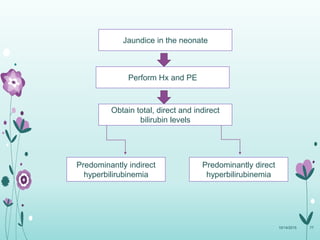
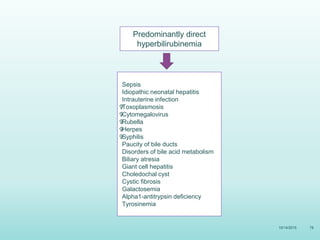
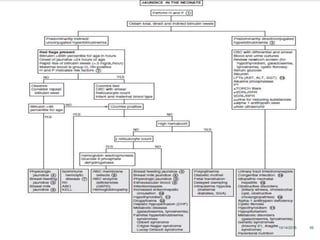
This document discusses the approach to jaundice and hyperbilirubinemia in newborns. It describes that hyperbilirubinemia is usually caused by increased bilirubin production, reduced hepatic uptake or conjugation, or decreased excretion. Jaundice appears as a yellow discoloration of the skin and progresses in a cephalocaudal pattern as bilirubin levels rise. Predominantly indirect hyperbilirubinemia is evaluated for red flags and risk factors, while predominantly direct hyperbilirubinemia indicates further testing for immune-mediated or metabolic causes of jaundice. Physiologic, breastfeeding, and breast milk jaundice represent common benign etiologies






























![GROUP_5_NEONATAL_JAUNDICE_PAEDICS[1] FINAL WORK [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/group5neonataljaundicepaedics1finalworkautosaved-250722234843-baaf238e-thumbnail.jpg?width=640&height=640&fit=bounds)

































