Downloaded 14 times
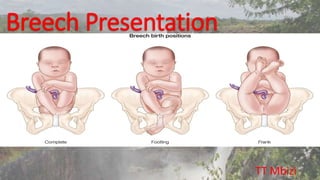
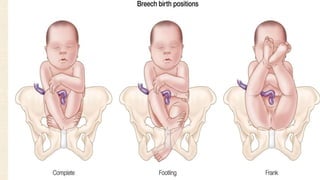
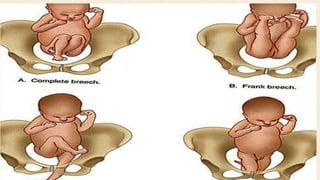
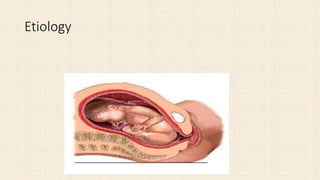

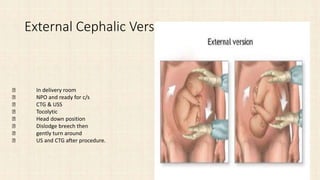


This document discusses breech presentation during pregnancy and delivery. It describes the causes of breech presentation as maternal factors like polyhydramnios or fetal factors like anomalies. It also outlines the diagnosis, management during pregnancy including external cephalic version, and delivery methods for breech presentation like vaginal delivery or cesarean section. Complications are discussed for both the mother and fetus.













![ANTEPARTUM HAEMORRHAGE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/antepartumhaemorrhageautosaved-230213084941-60834529-thumbnail.jpg?width=640&height=640&fit=bounds)