Downloaded 137 times

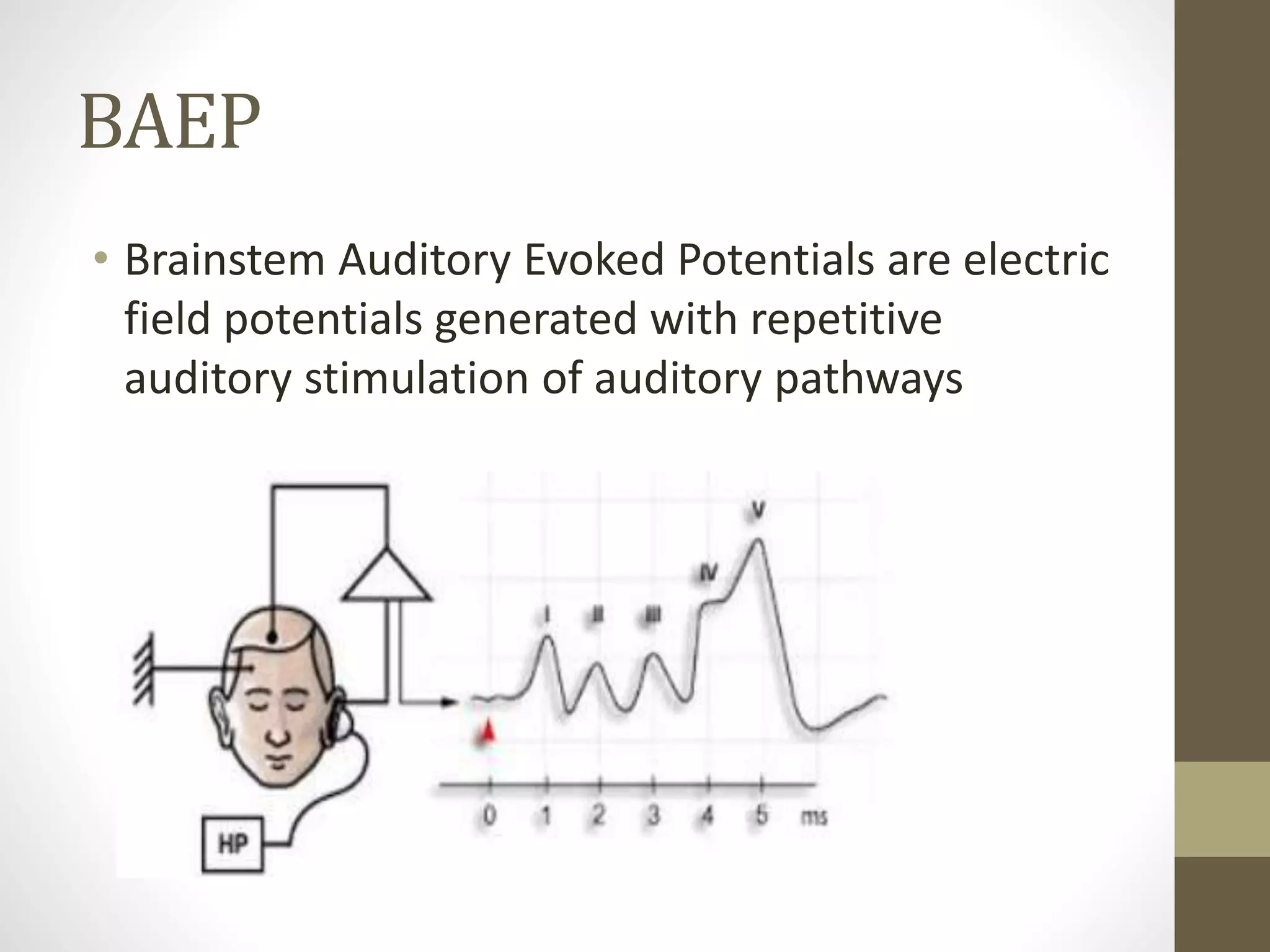














The document discusses the history and methodology of brainstem auditory evoked responses (BAER), highlighting key milestones and studies from 1967 onwards. It details the process of eliciting and recording BAERs, including electrode placement and stimulation techniques, as well as the interpretation of results. Additionally, it addresses clinical applications and variables that may influence BAER outcomes.



































































