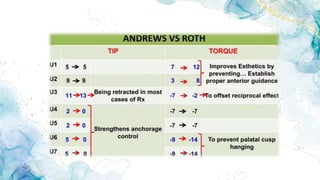
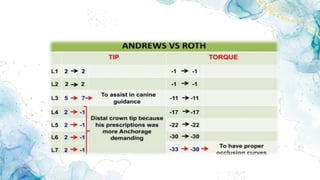
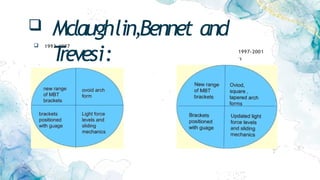
The document provides a comprehensive overview of orthodontic bracket prescriptions and their historical development, detailing the evolution from traditional appliances to modern pre-adjusted systems. It discusses the key concepts of order bends, normal occlusion, and the various contributions from pioneers like Andrews, Roth, and McLaughlin, highlighting their unique approaches to bracket design and orthodontic mechanics. Additionally, it covers hybridization techniques and the versatile applications of these orthodontic systems in practice.