Downloaded 206 times
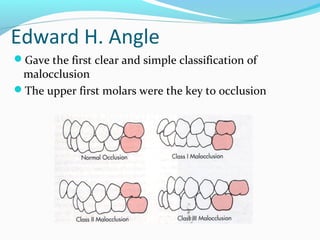
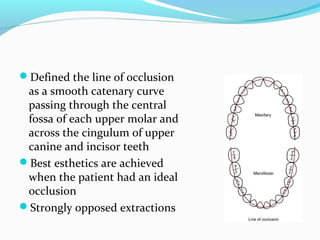
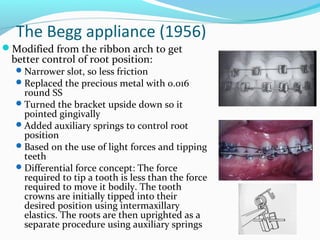

Edward H. Angle was a pioneering orthodontist who developed concepts of occlusion and malocclusion classification in the late 1800s. He opposed extracting teeth for orthodontic treatment. Several orthodontists further developed his ideas, creating new appliances like the Edgewise and Begg appliances to improve control of tooth movement and occlusion. In the 1970s, Larry Andrews identified characteristics of ideal occlusion from studying untreated ideal bites. He developed the preadjusted edgewise appliance and "Six Keys of Occlusion" to achieve optimal occlusion without wire bending. Ronald Roth built on Andrews' work by incorporating the temporomandibular joint.





![Loops in orthodontics and its uses [Autosaved]..ppt](https://cdn.slidesharecdn.com/ss_thumbnails/loopsinorthodonticsautosaved-241204161830-0e1eccec-thumbnail.jpg?width=640&height=640&fit=bounds)















































































