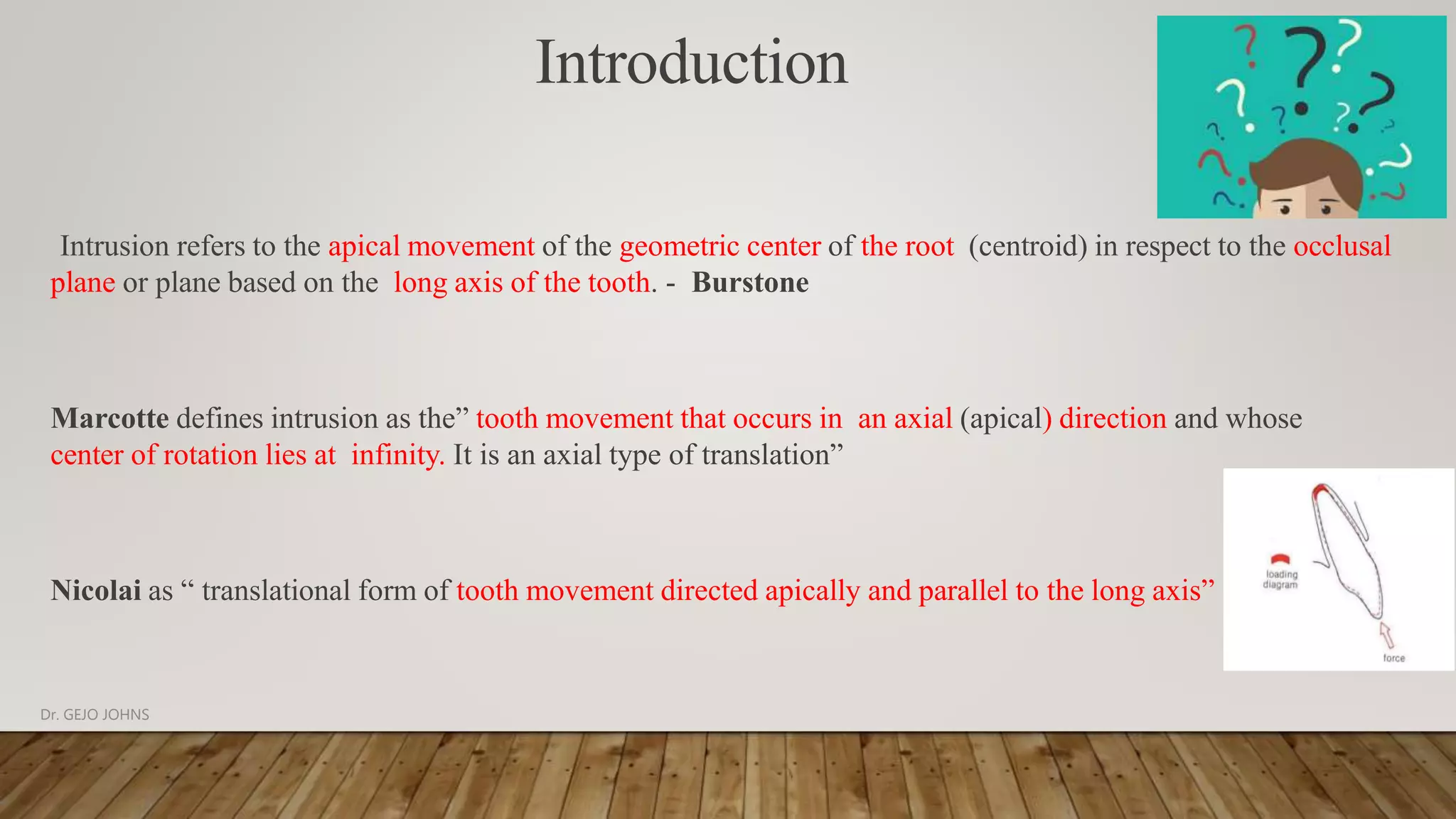
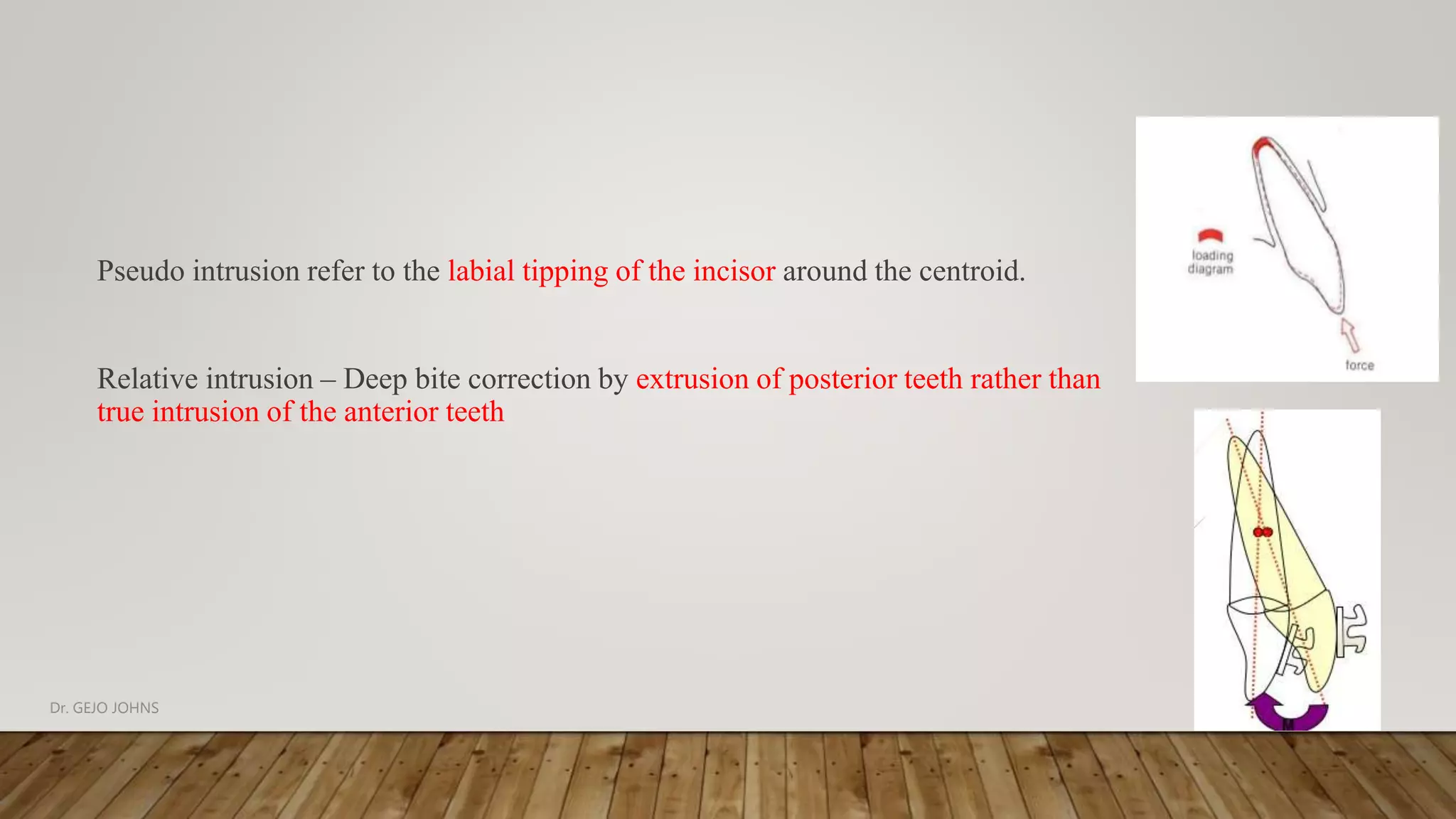
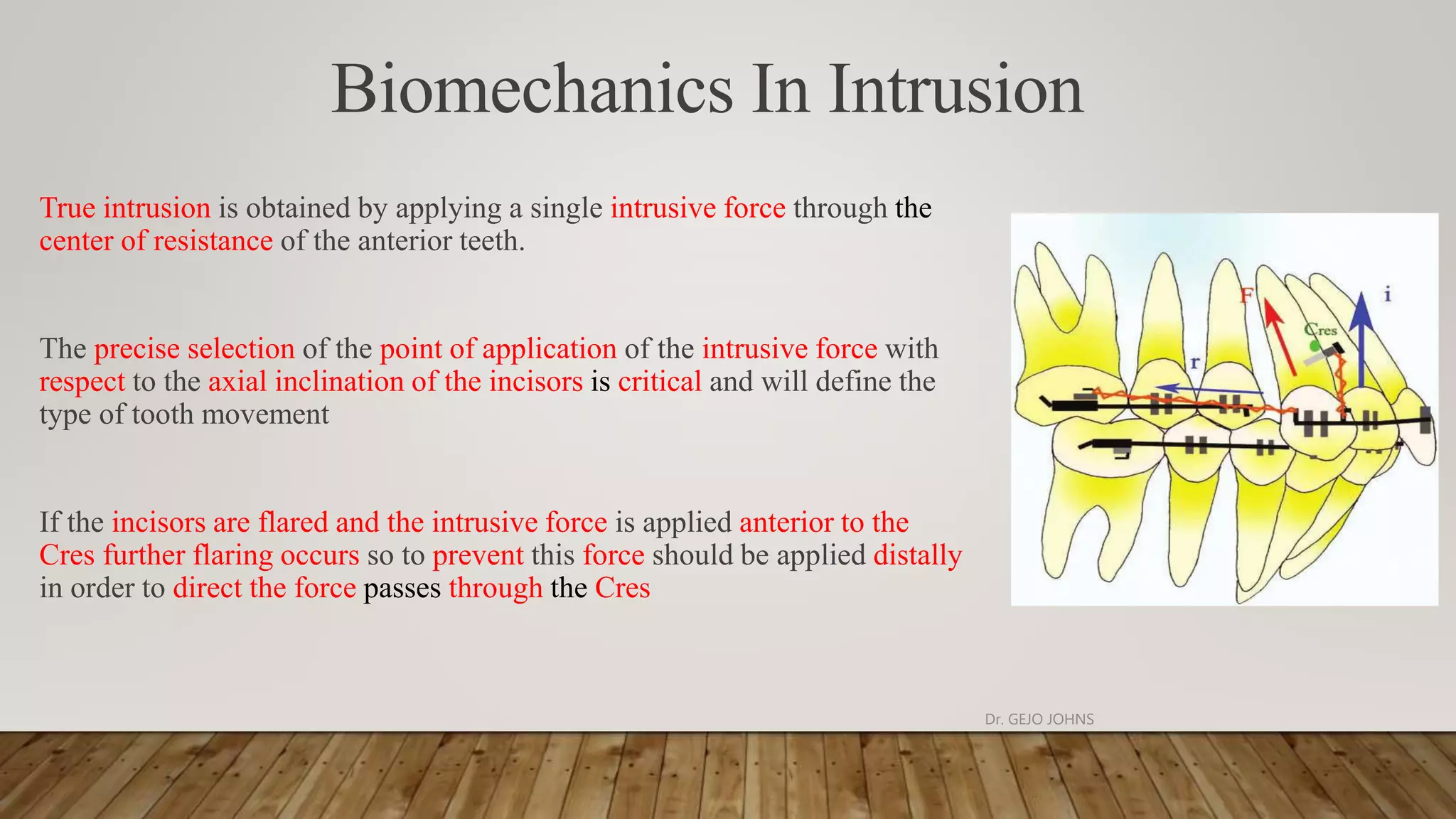
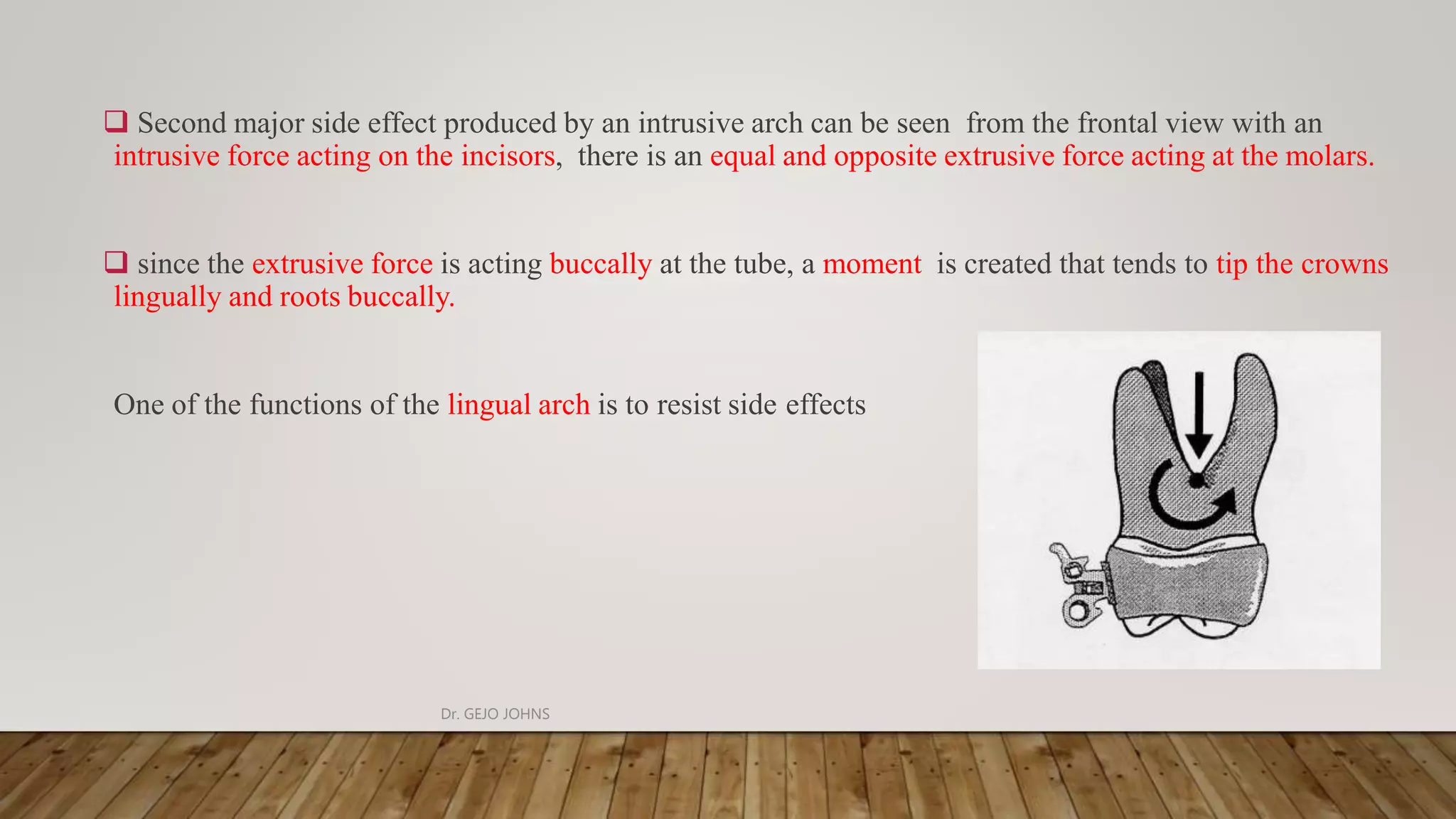
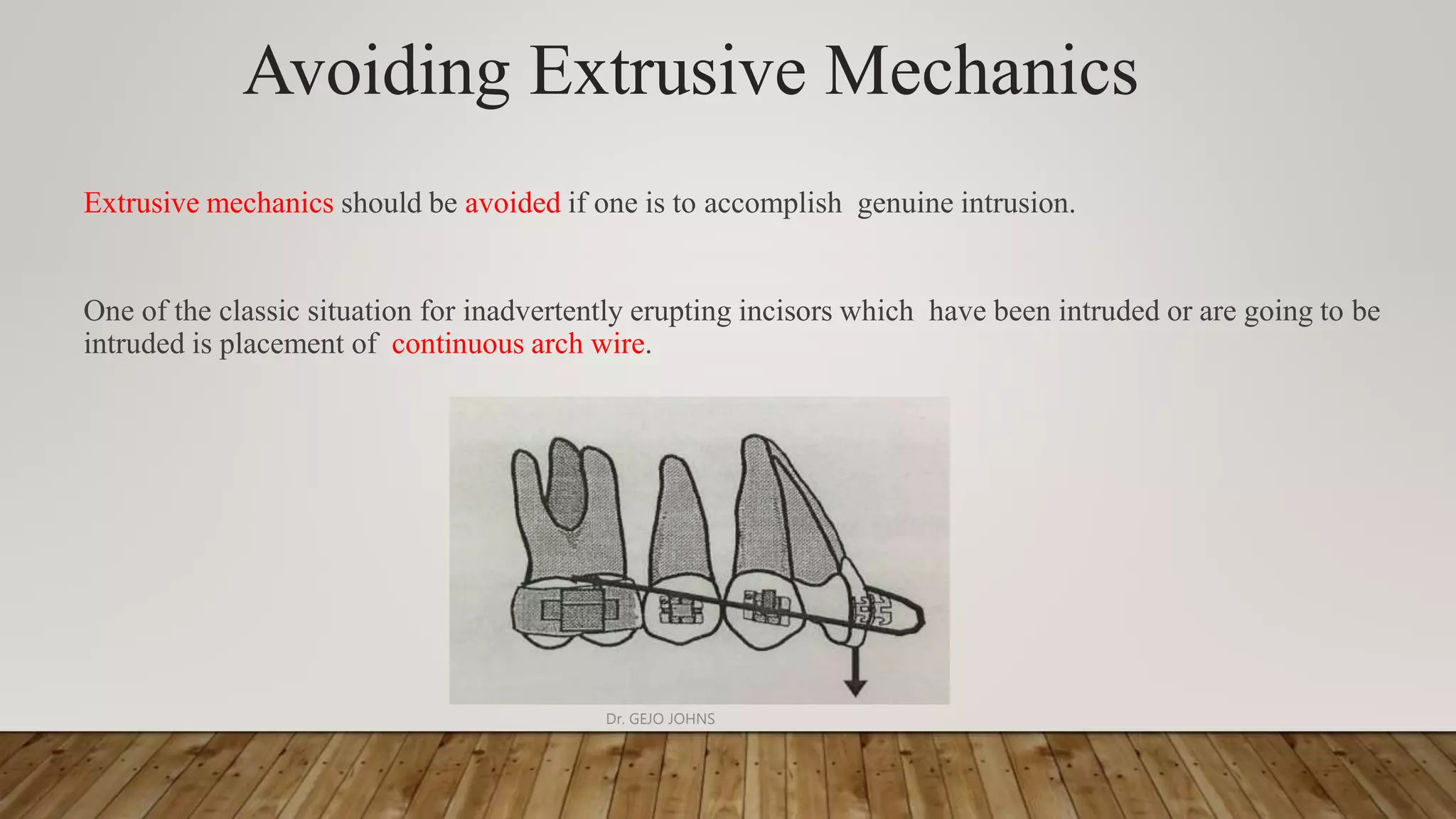
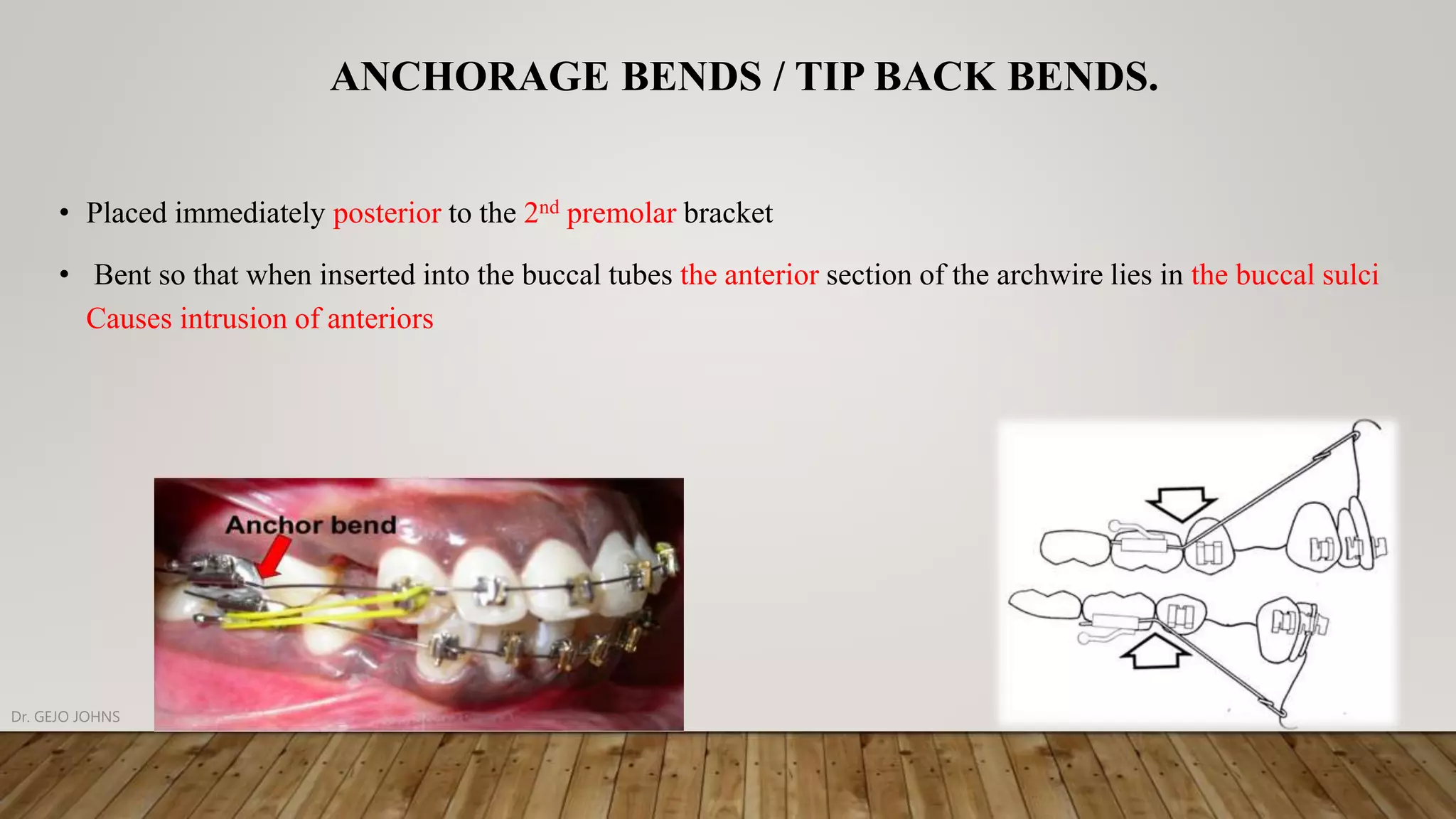
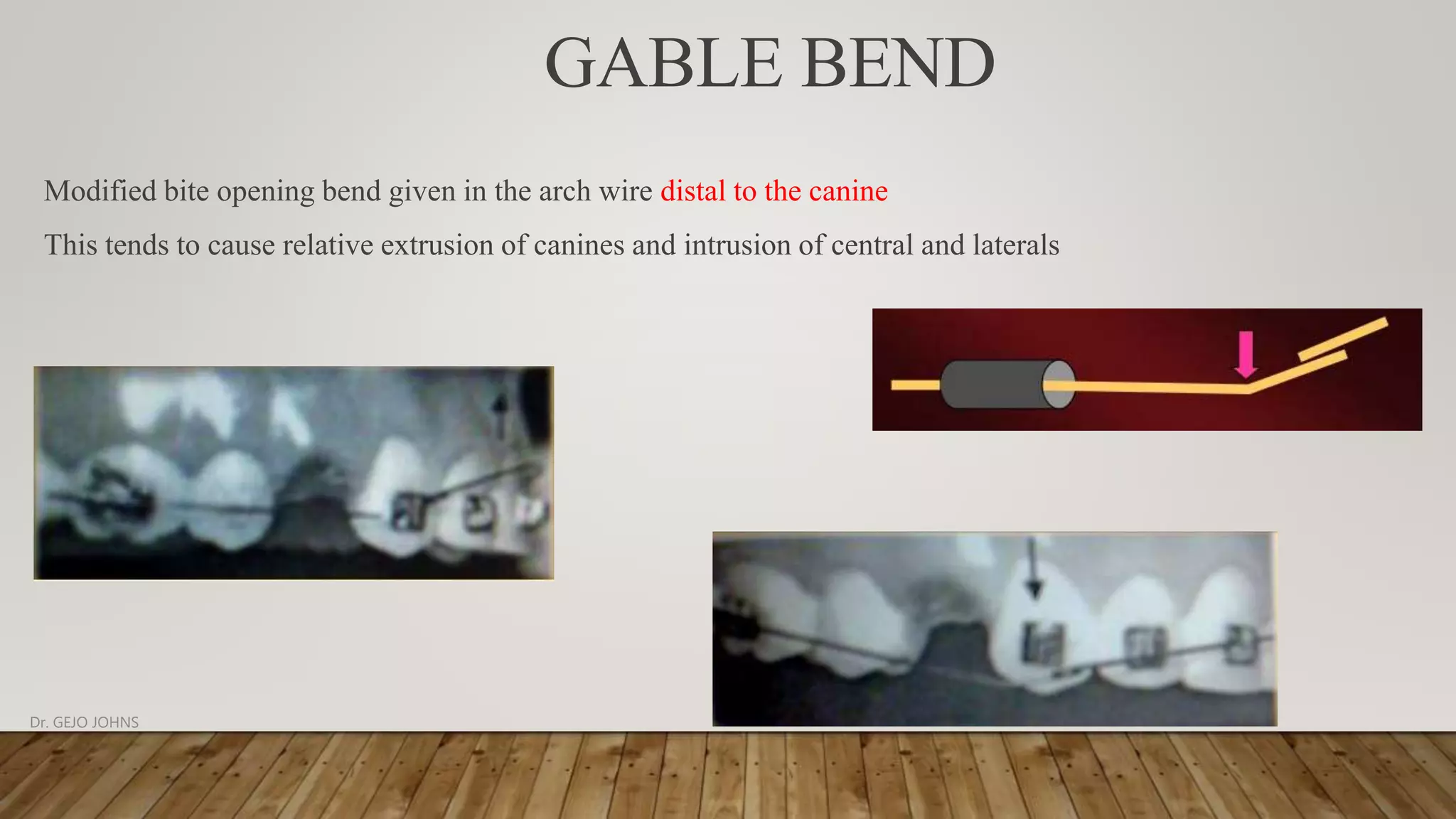
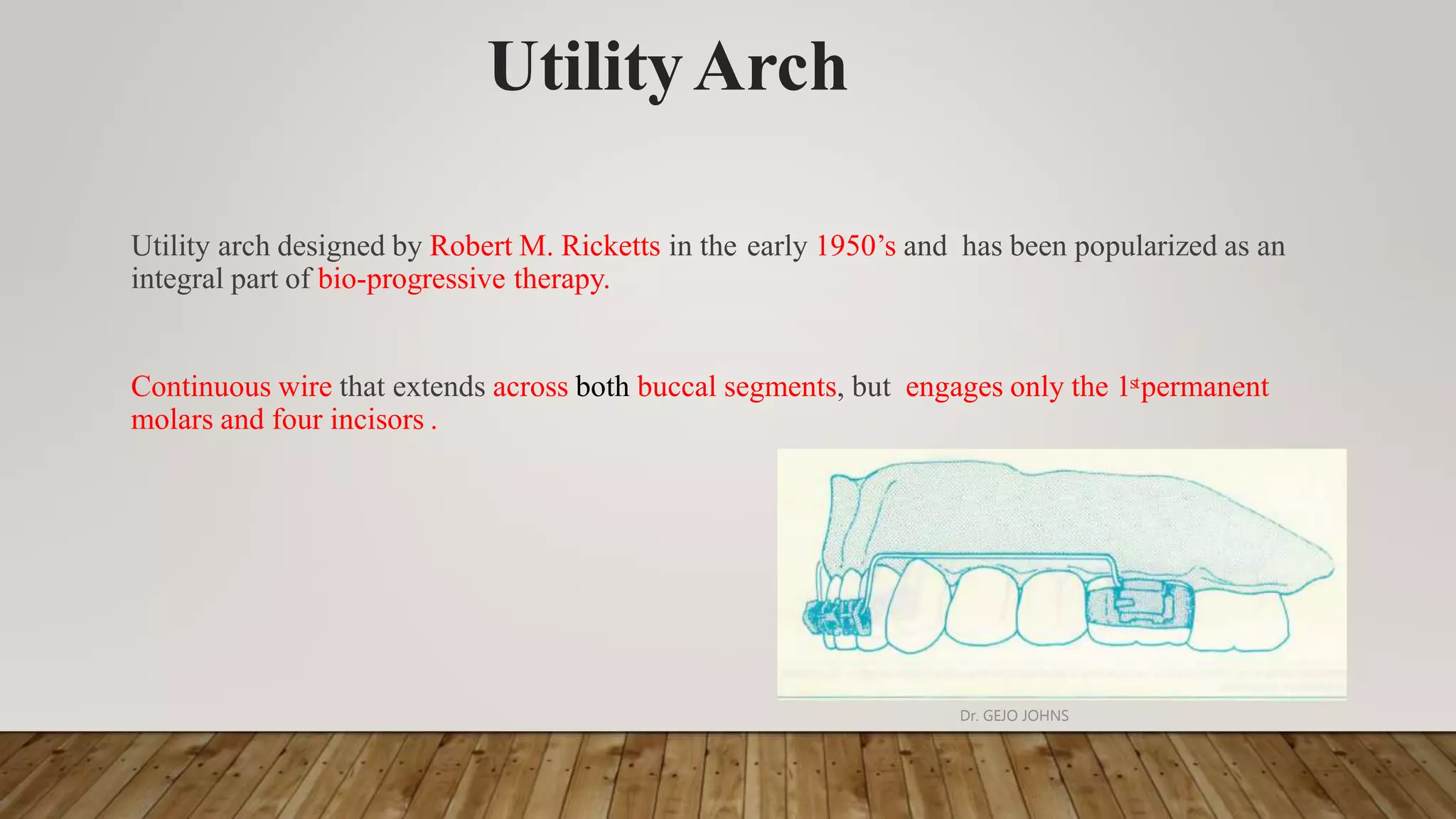
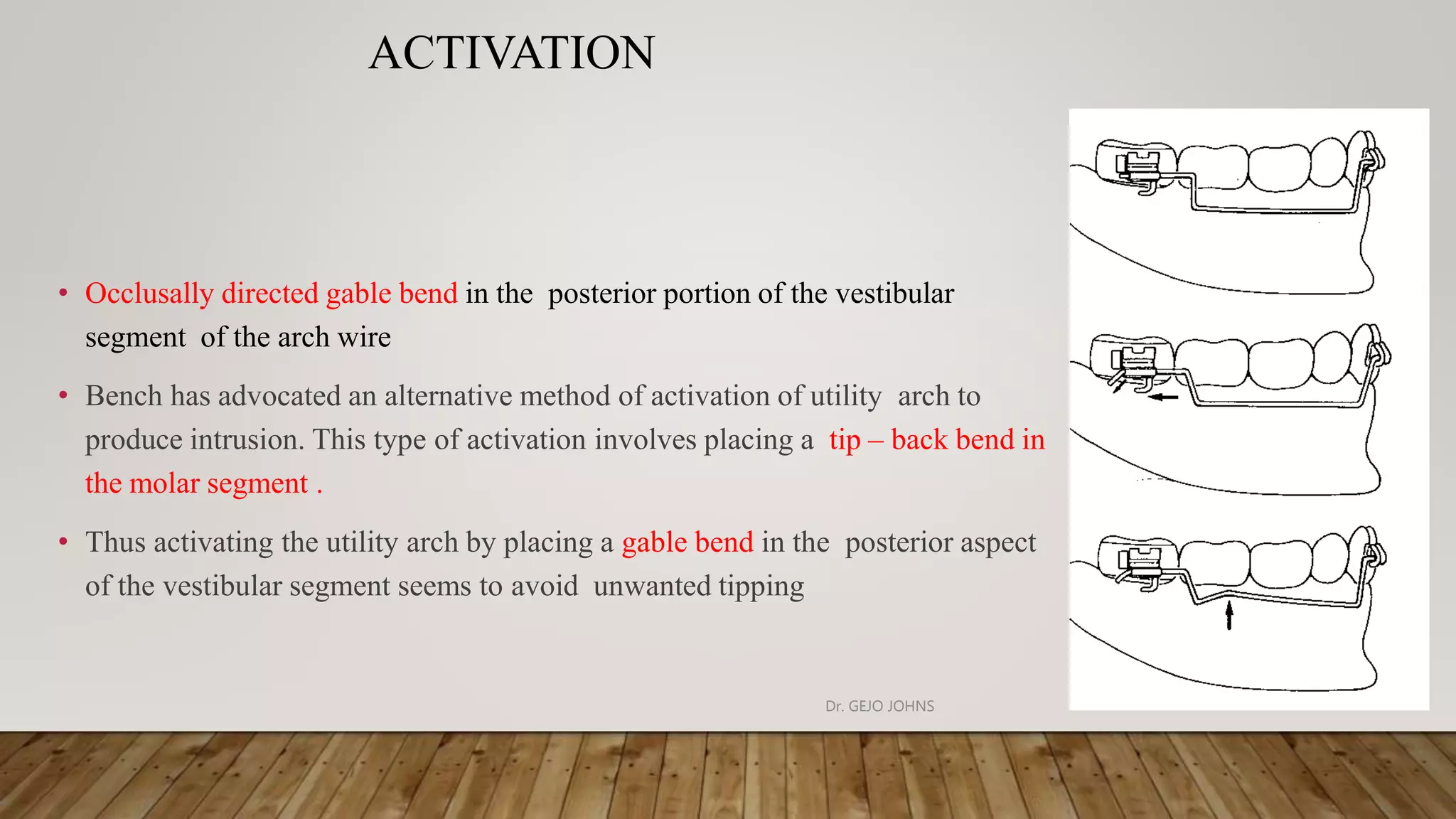
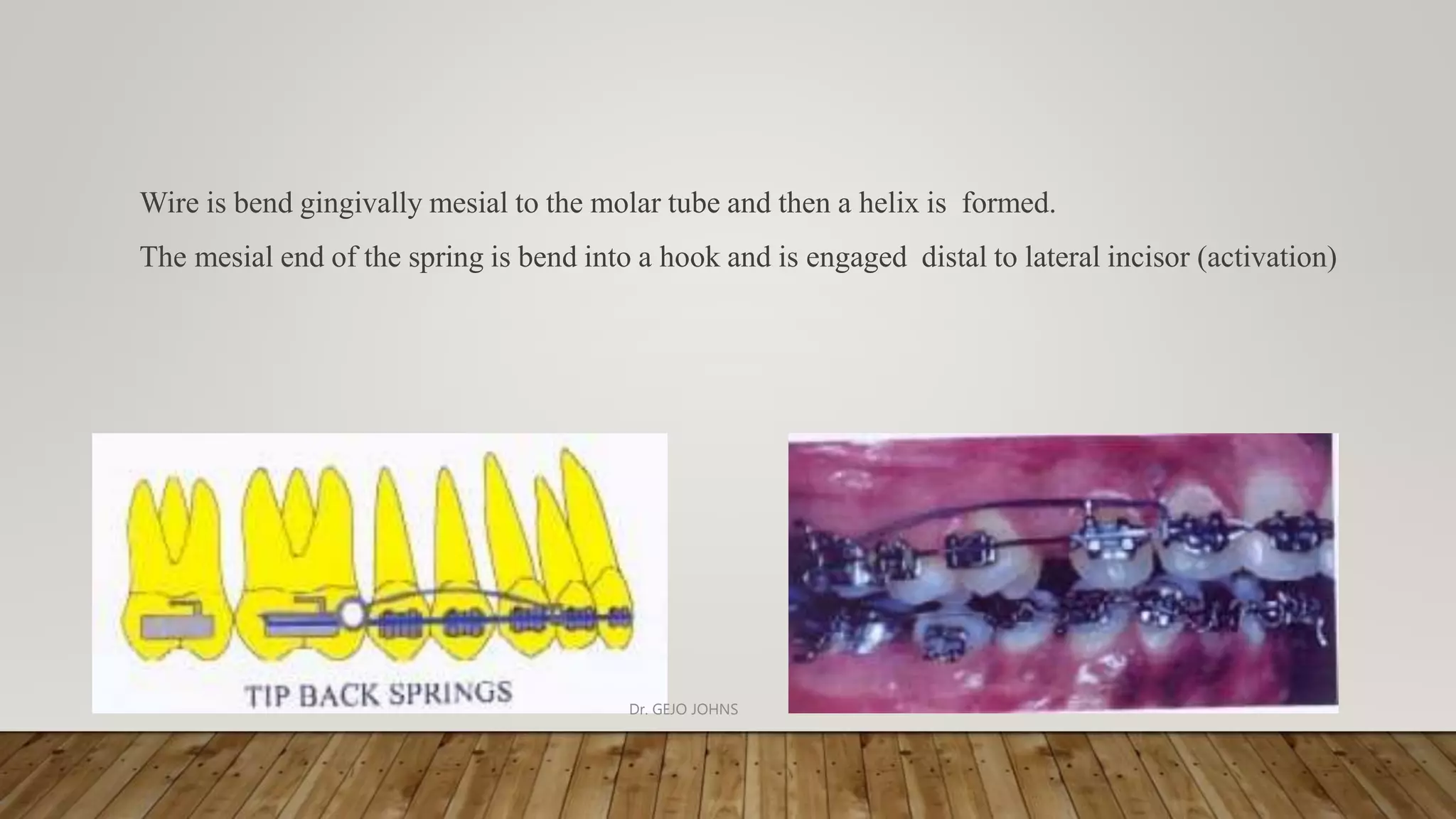
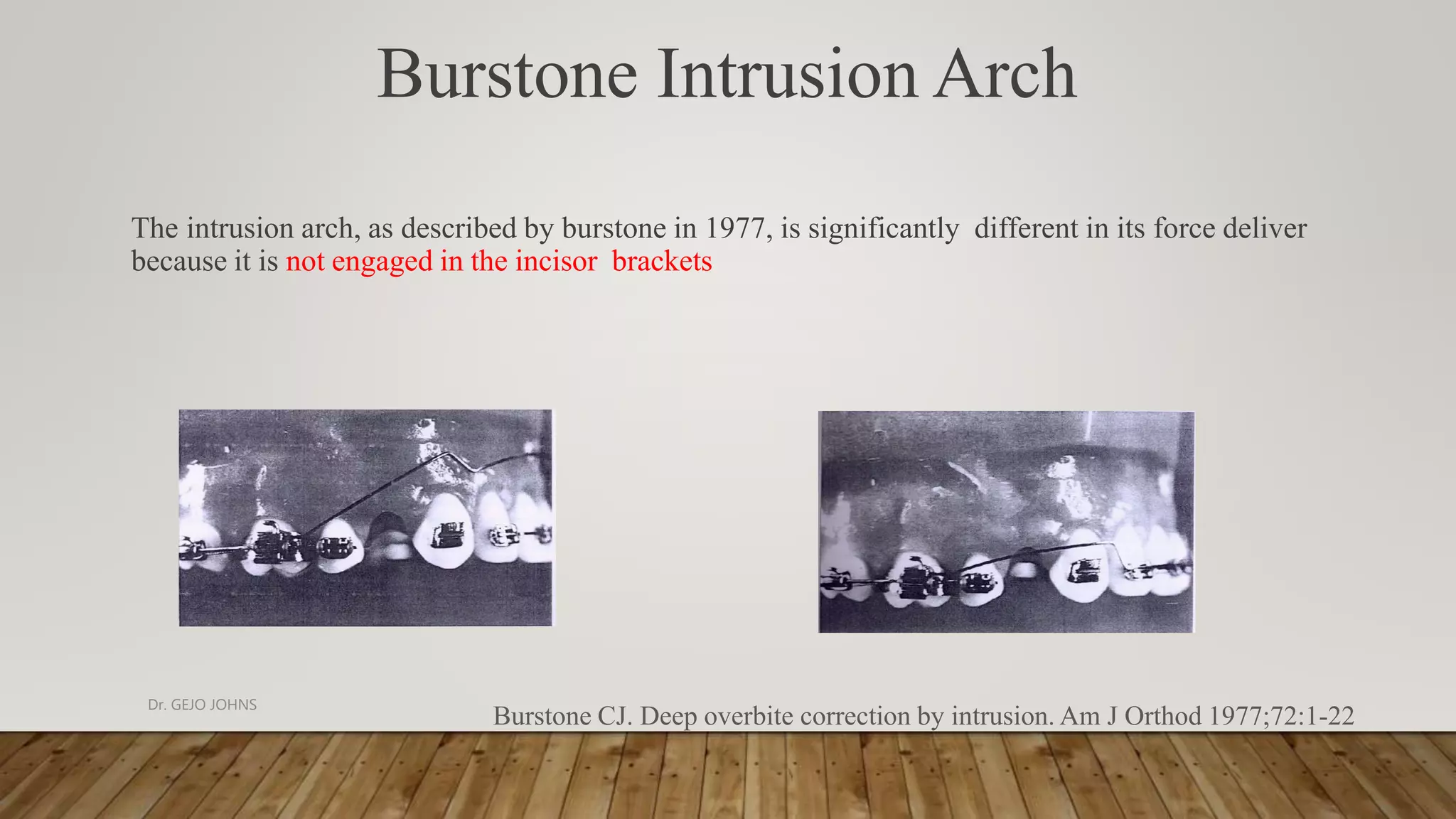
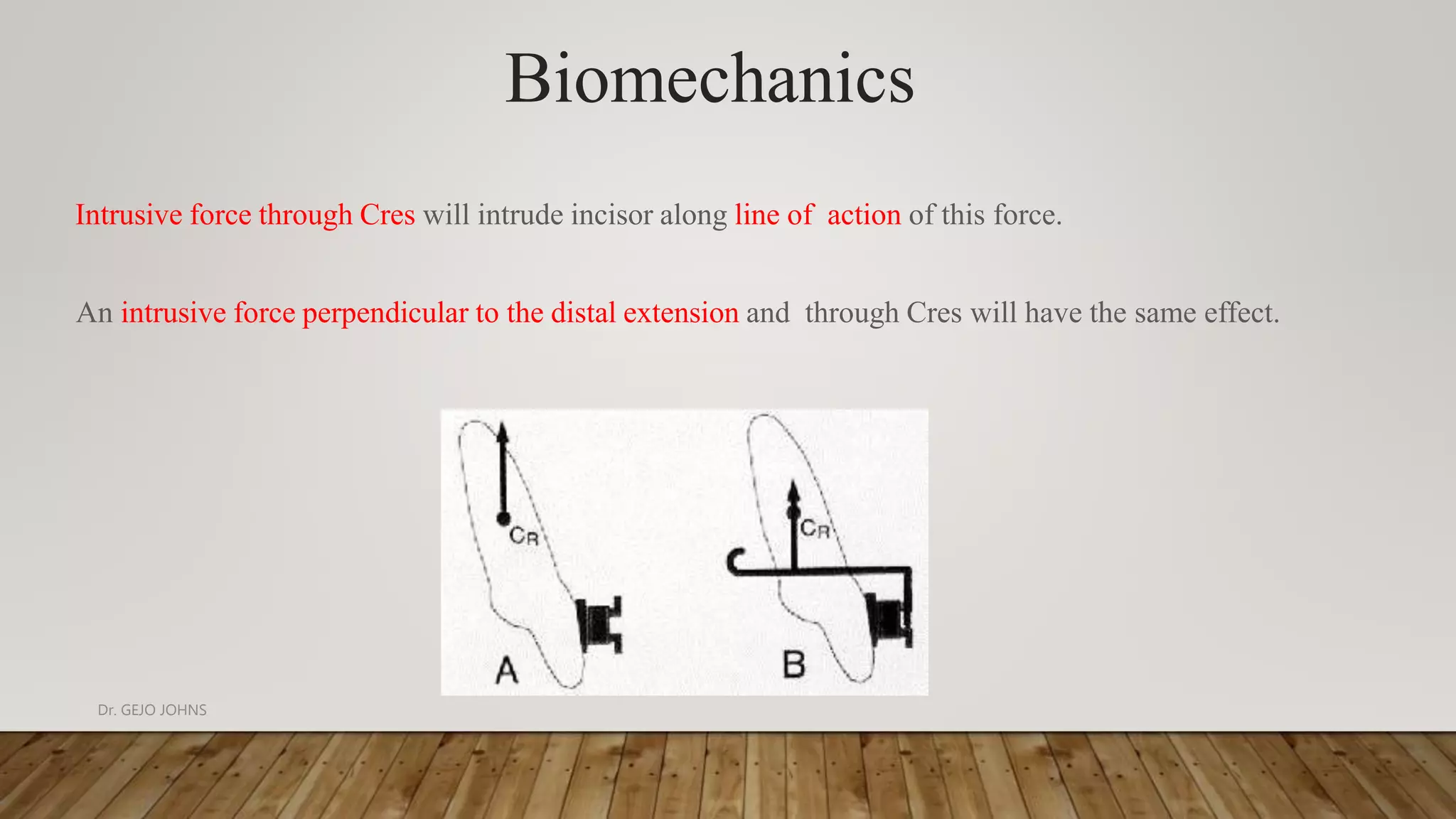
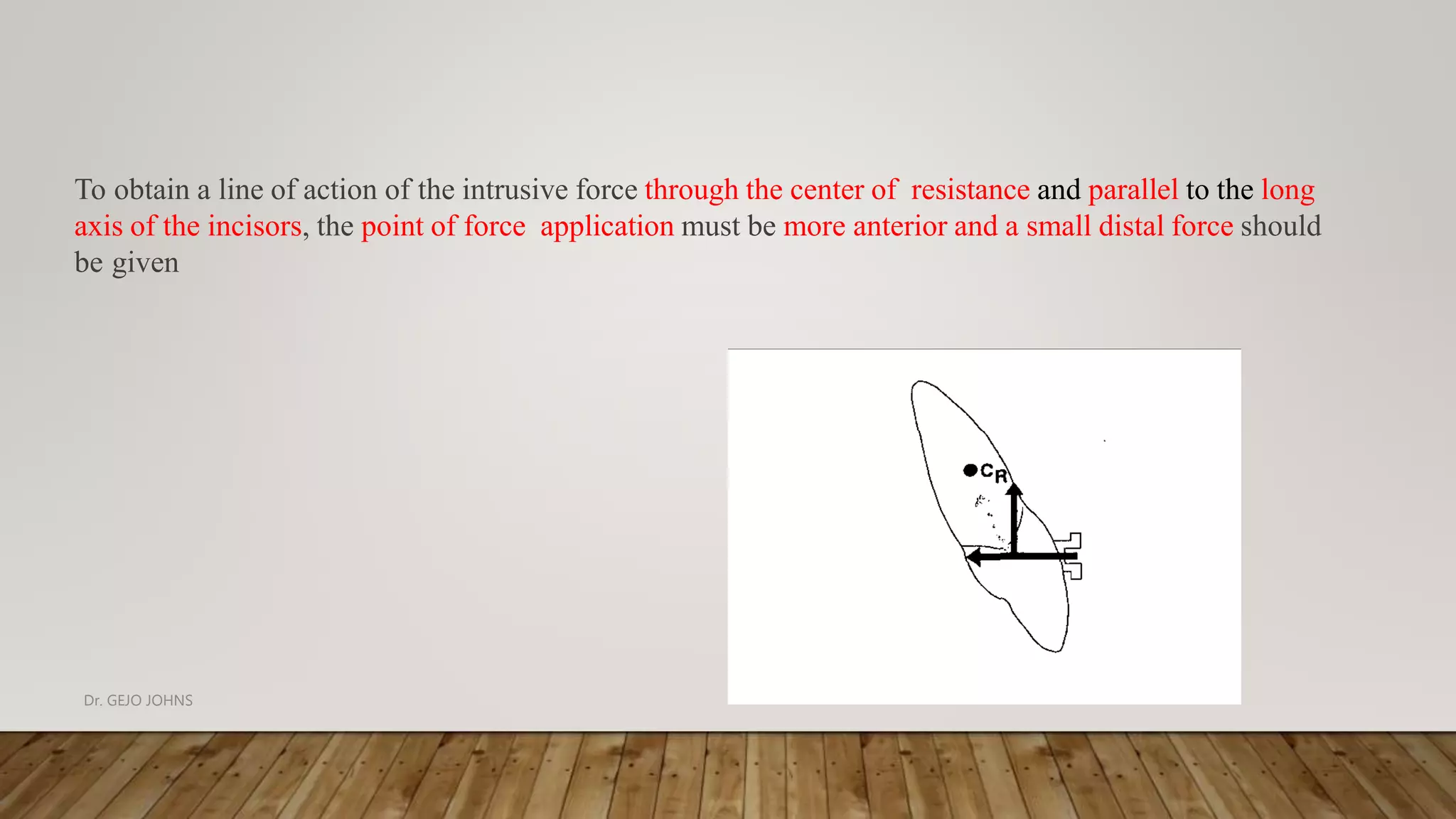
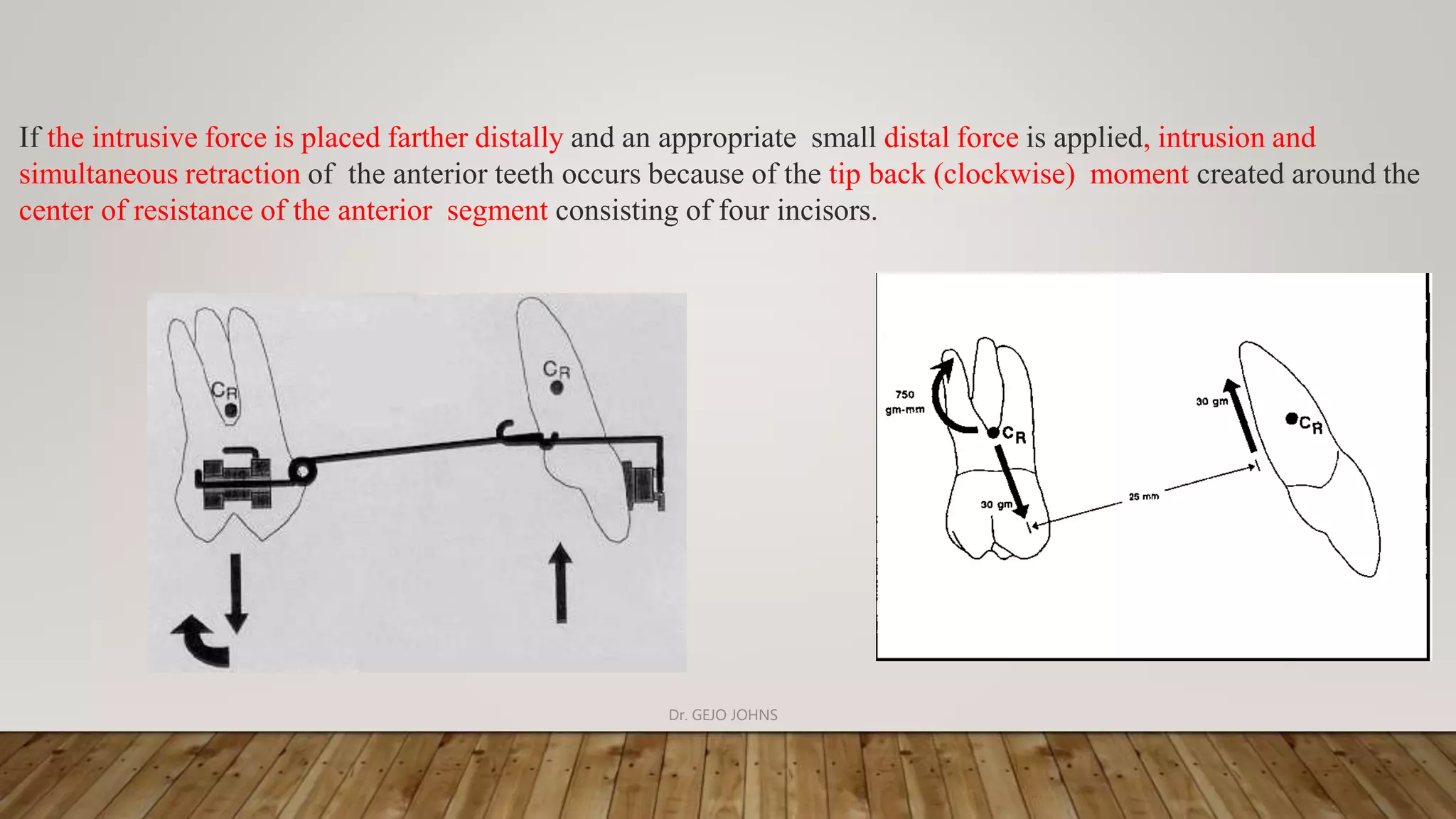
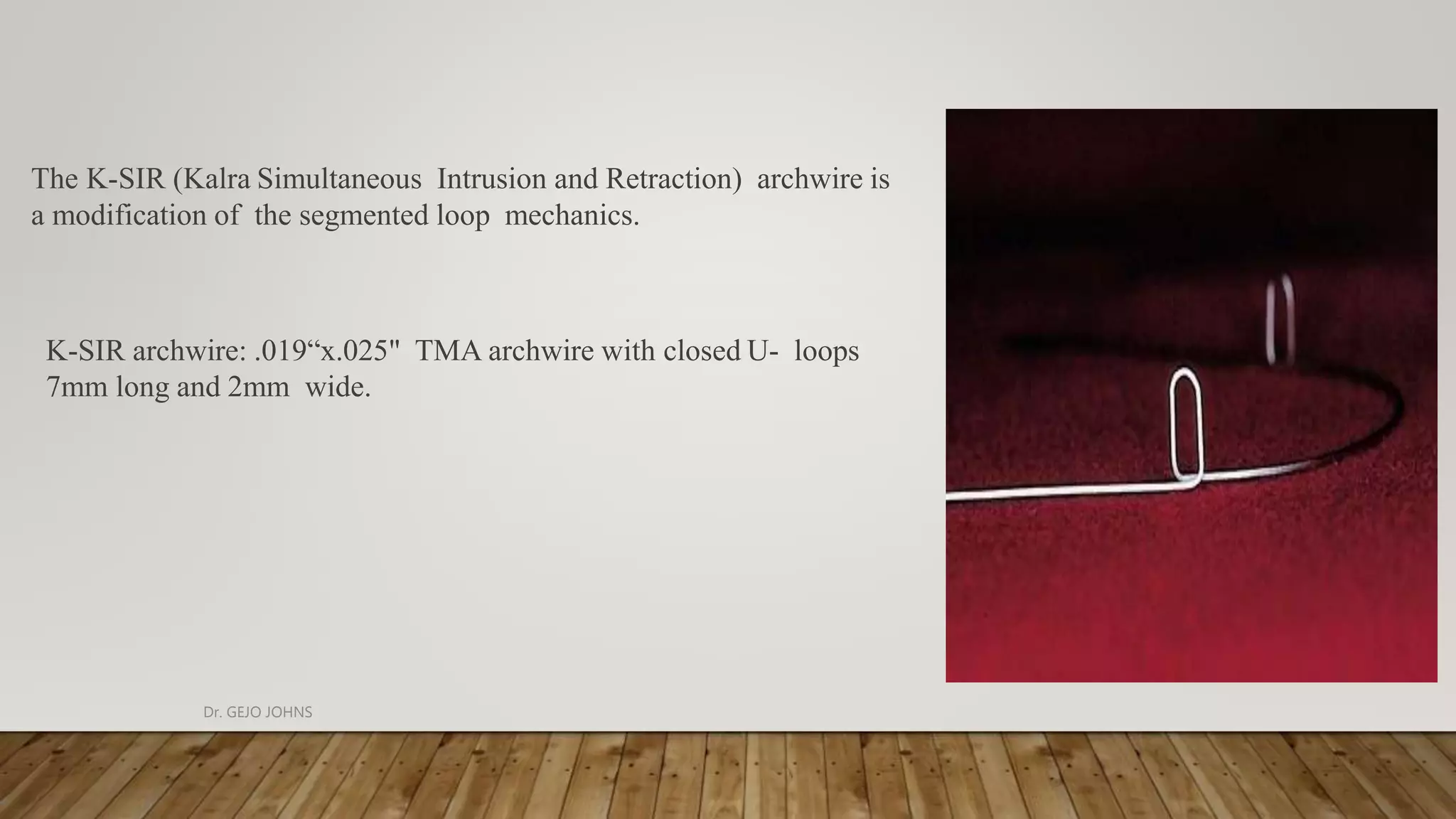
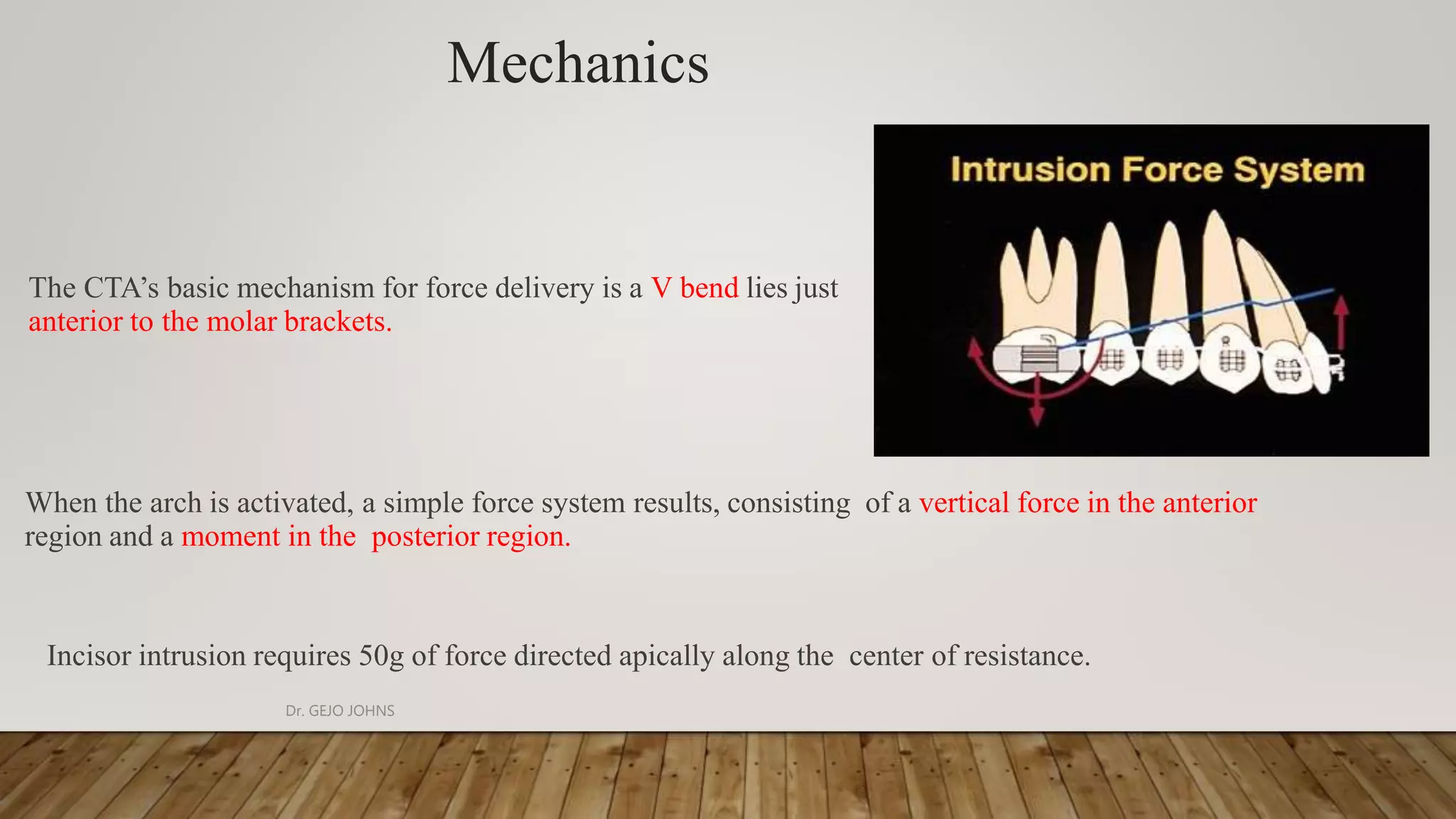
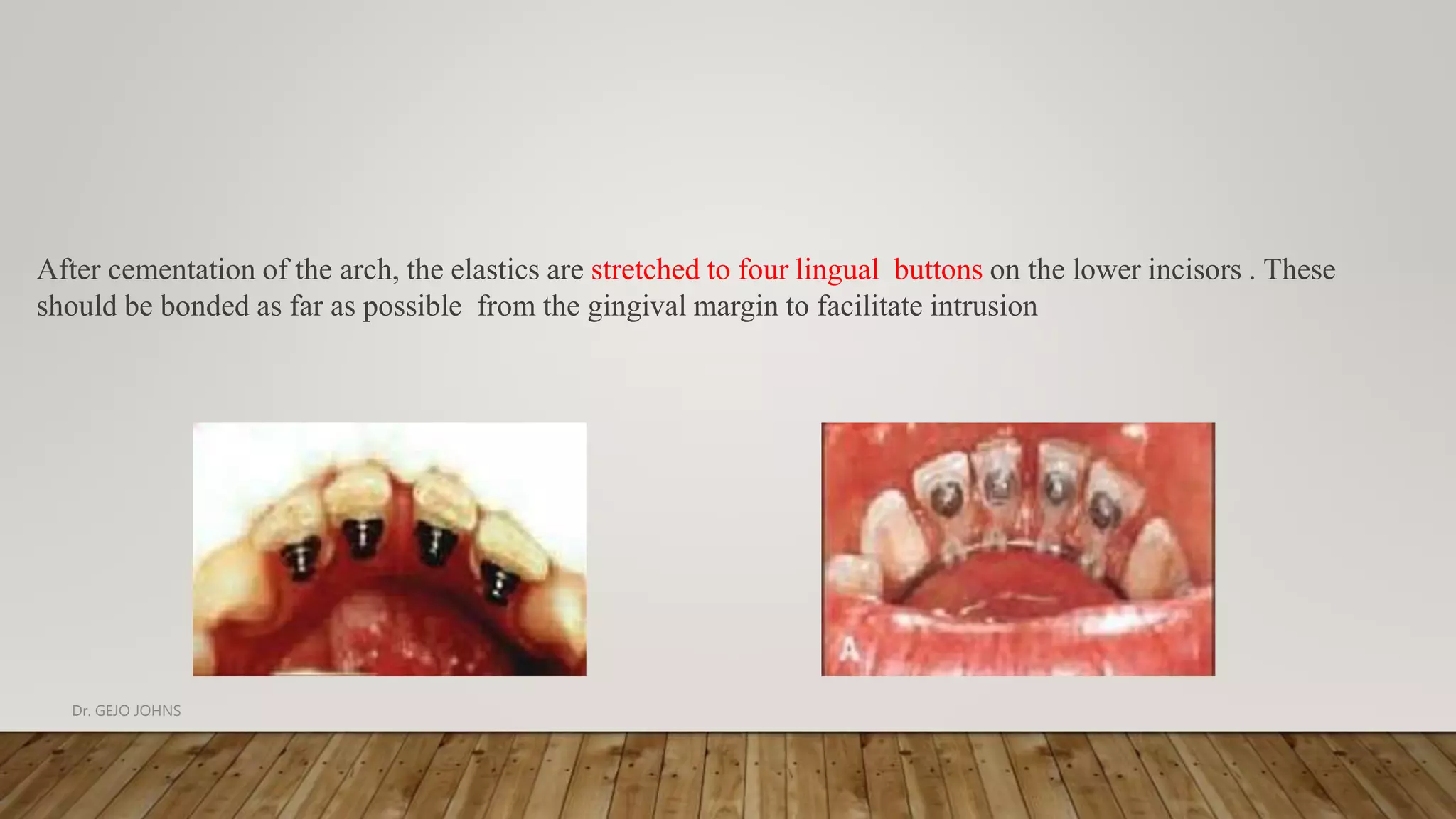
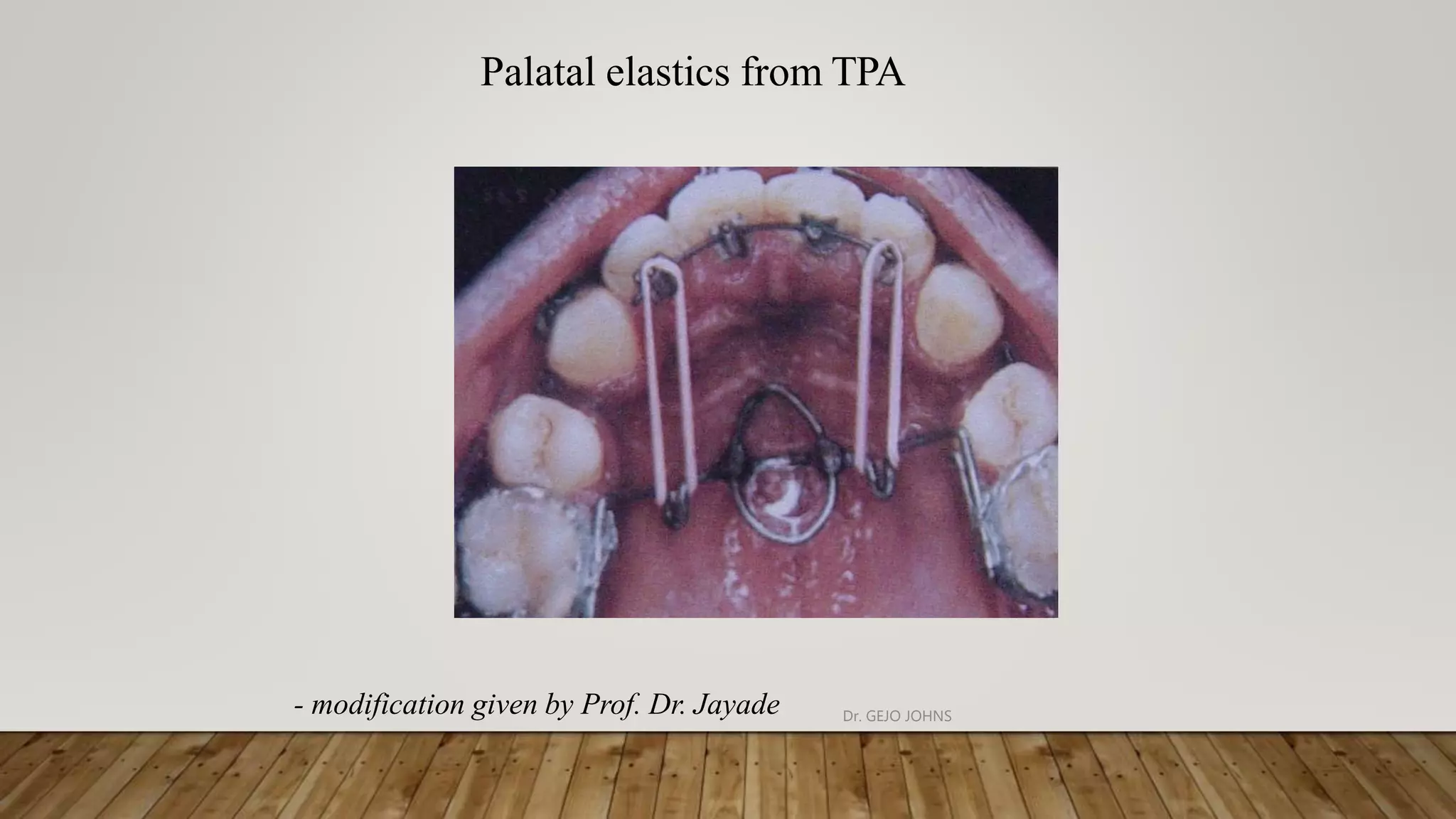
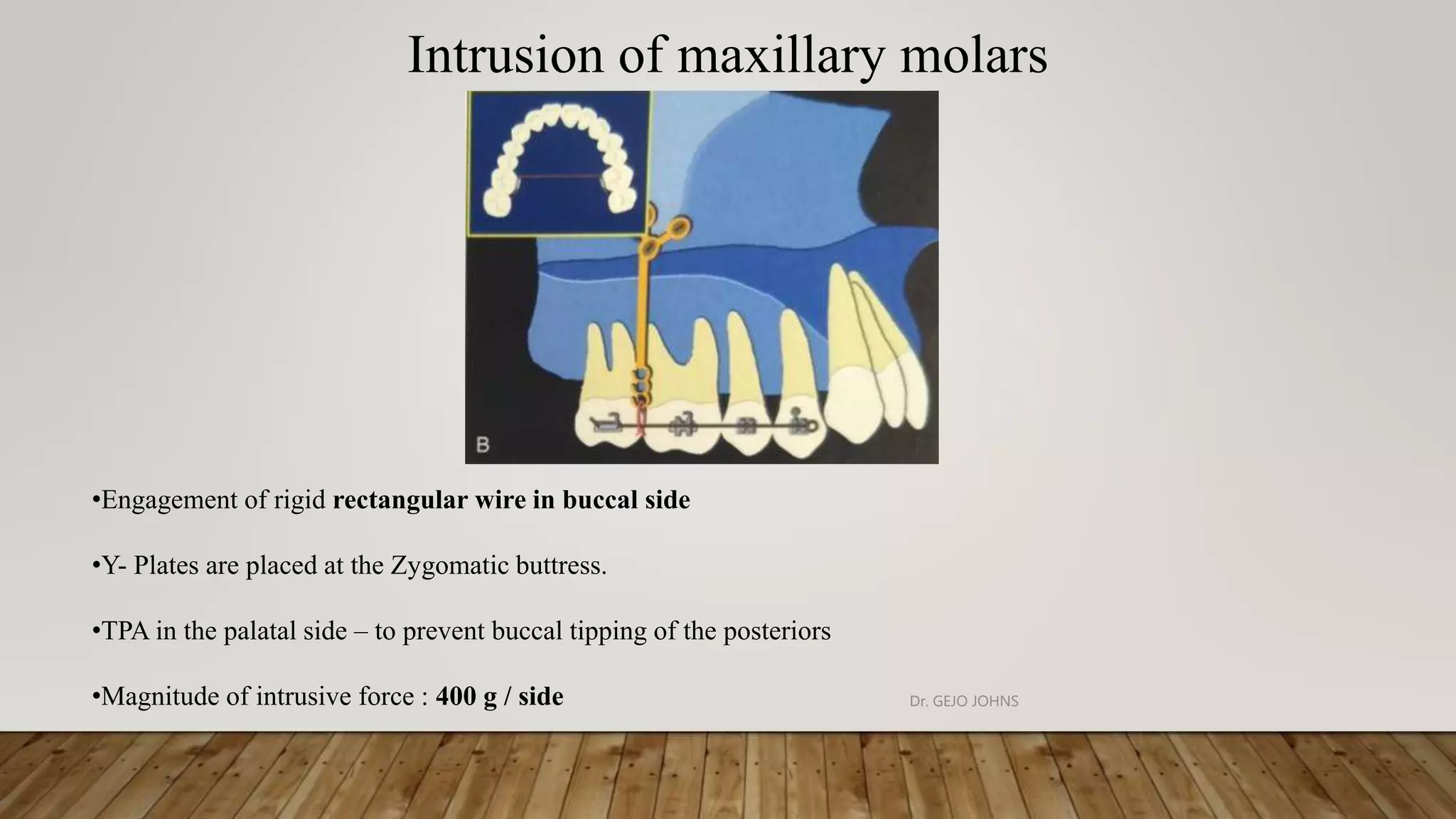
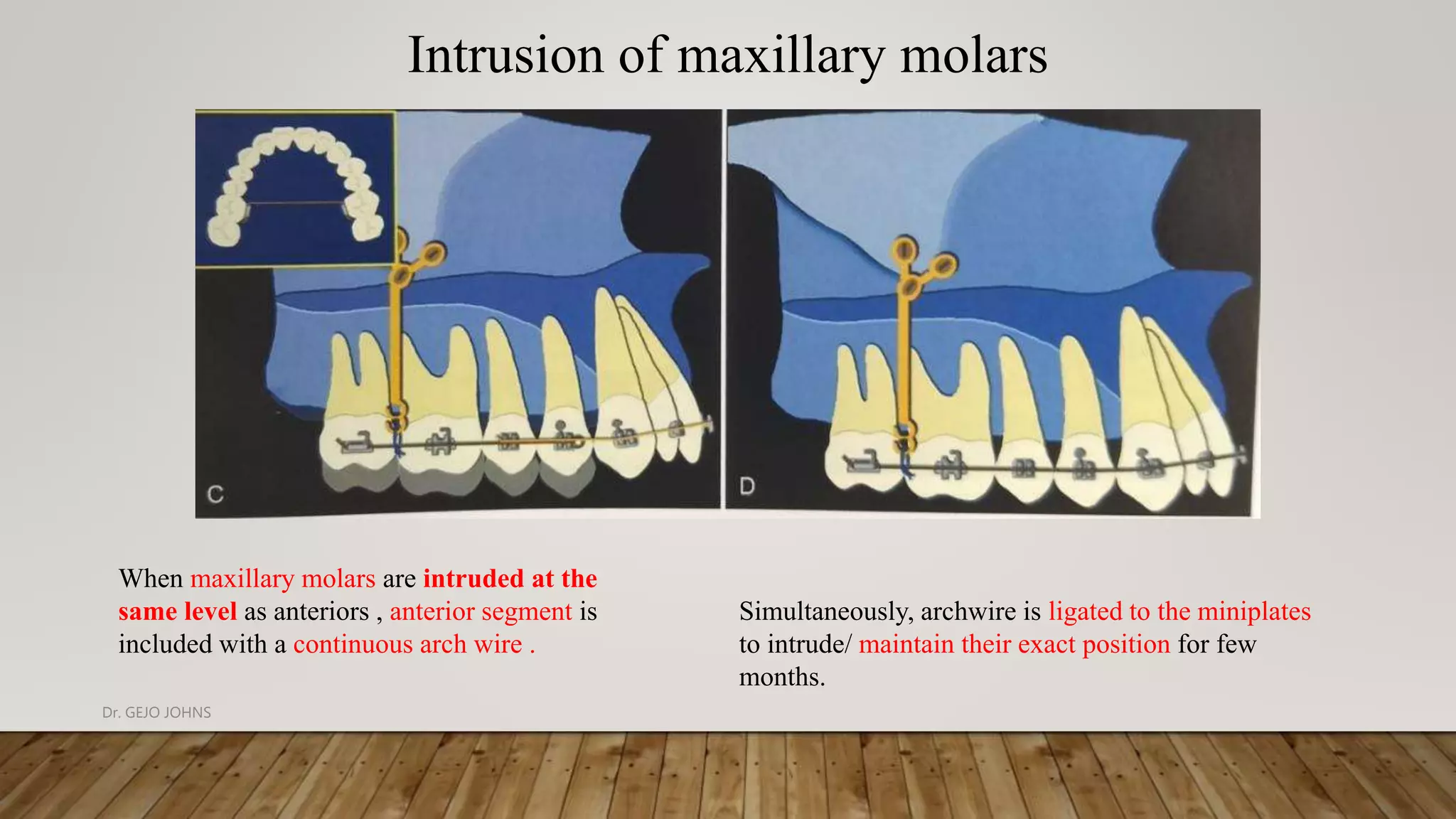
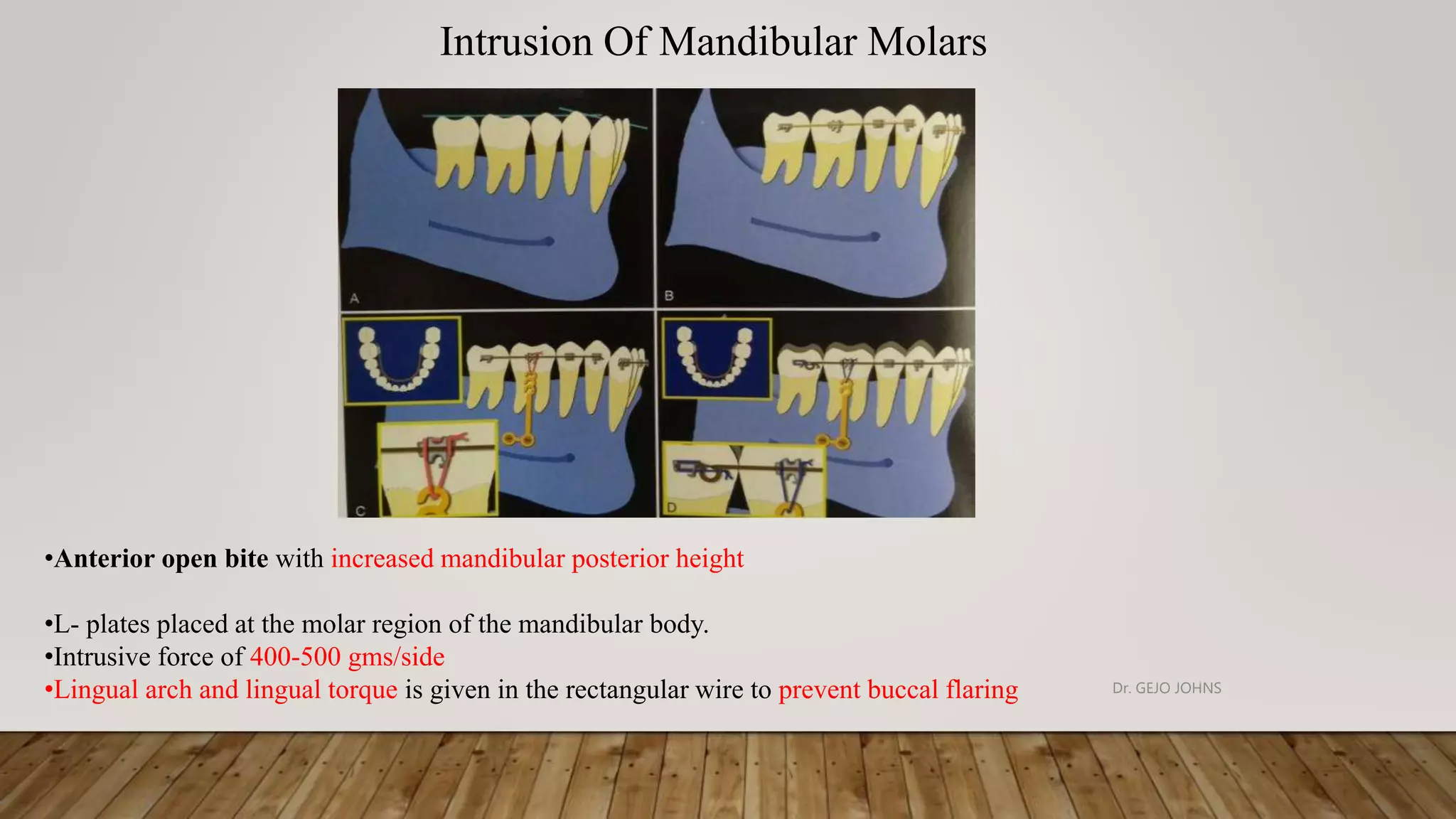
This document discusses various techniques for intruding teeth in orthodontics. It begins by defining intrusion and describing how it differs from other tooth movements like tipping. Deep overbites can be corrected through intrusion of anterior teeth or other movements. The principles of intrusion mechanics include applying light continuous forces through the center of resistance and using devices that create statically determinate force systems. Various intrusion appliances are described, including utility arches, tipback springs, continuous and segmented intrusion arches. Key biomechanical concepts for intrusion like controlling reactive forces and avoiding extrusion are also summarized.