
Recommended
More Related Content
Similar to BENIGN PROSTATIC HYPERPLASIA.pptx
Similar to BENIGN PROSTATIC HYPERPLASIA.pptx (20)
Recently uploaded
Recently uploaded (20)
BENIGN PROSTATIC HYPERPLASIA.pptx
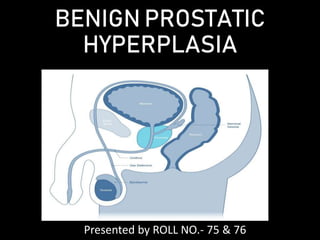
- 1. BENIGN PROSTATIC HYPERPLASIA Presented by ROLL NO.- 75 & 76
- 2. Anatomy Embryology Develops around 12th week of intra uterine life . Primitive buds from urethra form glandular tissue . Surrounding mesenchyme forms the fibromuscular stroma . • Developmentally prostate has 5 lobes- anterior ,posterior , middle and 2 lateral lobes.
- 3. • Enlargement of middle lobe / median lobe in BPH is responsible for urethral obstruction. It enlarges upwards into the bladder . In BPH glands of inner adenomatous zone hypertrophies – leads to obstruction. Carcinoma occurs in outer non- adenomatous zone ( posterior lobe ).
- 4. Zones of prostate Based on McNeal’s zonal anatomy – 5 zones have been identified 1. Central zone 2. Periurethral glandular tissue 3. Transitional zone 4. Peripheral zone 5. Anterior fibromuscular stroma
- 5. Structural anatomy- verumontanum Prostatic urethra is surrounded by fibroadenomatous gland Urethral glands open into prostatic urethra . These submucosal glands are responsible for BPH . When prostate enlarges it compresses the outer zone resulting in false capsule .
- 6. BPH- DEFINITION: • Non cancerous increase in size of prostate gland which involves hyperplasia of prostatic stromal & epithelial cell resulting in formation of large fairy discrete nodule in transitional zone of prostate ,which push on and narrow the urethra resulting in an increase resistance to flow of urine from the bladder.’’
- 8. INCIDENCE: • Occurs in men over 50 years of age; by the age of 60 years, 50% of men have histological evidence of BPH • Common cause of significant lower urinary tract symptoms in men and is the most common cause of bladder outflow obstruction in men > 70 years of age
- 9. AETIOLOGY: • Serum testosterone levels slowly but significantly decrease with advancing age; however, levels of oestrogenic steroids are not decreased equally. • According to this theory, the prostate enlarges because of increased oestrogenic effects. That the secretion of intermediate peptide growth factors plays a part in the development of BPH
- 10. PATHOLOGY: • BPH affects both glandular epithelium and connective tissue • Typically affects the submucous group of glands in the transitional zone, forming a nodular enlargement. Eventually, this overgrowth compresses the PZ glands into a false capsule and causes the appearance of the typical ‘lateral’ lobes. • When BPH affects the subcervical CZ glands, a ‘middle’ lobe develops that projects up into the bladder within the internal sphincter. • Sometimes, both lateral lobes also project into the bladder, so that, when viewed from within, the sides and back of the internal urinary meatus are surrounded by an intravesical prostatic collar
- 12. EFFECTS OF BENIGN PROSTATIC HYPERPLASIA Pathophysiologically, BOO may be caused in part by increased smooth muscle tone, which is under the control of α-adrenergic agonists
- 13. ANATOMICALLY: EFFECTS • Urethra- The prostatic urethra is lengthened, sometimes to twice its normal length, but it is not narrowed anatomically. The normal posterior curve may be so exaggerated that it requires a curved catheter to negotiate it. When only one lateral lobe is enlarged, distortion of the prostatic urethra occurs. • Bladder- If BPH causes BOO, the musculature of the bladder hypertrophies to overcome the obstruction and appears trabeculations / fasciculations . • Between the fasciculations , depressed area called sacculations. • Sacculi are thin as pressure increasee, herniation occurs outside, resulting in diverticuli.
- 14. • Ureter & Kidney- bilateral hydronephrosis and bilateral hydroureter are the end result of BPH , may result in renal failure .
- 15. CLINICAL FEATURES: • FREQUENCY , URGENCY & HESITANCY- TRIAD OF BPH. BPH IRRITATIVE SYMPTOM FREQUENCY URGENCY NOCTURIA OBSTRUCTIVE SYMPTOM POOR STREAM INTERMITTENCY STRAINING SENSE OF INCOMPLETE EMPTYING MNEMONIC: FUN PISS
- 16. • FREQUENCY: Present in daytime followed by night (5-10 times) it is due to ineffective emptying of bladder , results in residual urine in bladder and precipitate cystitis. • URGENCY: Vesical introversion of the sensitive mucus membrane of the prostatic urethra within the bladder. This causes the internal sphincter to stretch and prevents contraction. Resulting in a few drops of urine trickling down the posterior urethra , causing an urgent desire to pass urine (urgency) • HESITANCY :Hesitation to pass urine because obstruction makes it ineffective. • HEMATURIA (rare): Due to congestion of the prostatic venous plexuses resulting in hyperemia and hematuria.
- 17. • ACUTE RETENTION OF URINE: Sometime first symptom of BOO. This occurs due to postponement of micturition ,following alcohol or drugs like mydriatics. • CHRONIC RETENTION: In patients in whom the residual volume is > 250 ml or so, the tension in the bladder wall increases owing to the combination of a large volume of residual urine and increased resting and filling bladder pressures (a condition known as high- pressure chronic retention). • The increased intramural tension results in functional obstruction of the upper urinary tract with the development of bilateral hydronephrosis.
- 18. COMPLICATIONS - • STONES: 8 times more common • DIVERTICULI • RENAL FAILURE • RECURRENT UTI : Most common cause of surgical intervention.
- 19. DIAGNOSIS OF BPH: • DIGITAL RECTAL EXAMINATION: Enlarged lateral lobes can be easily felt. Rectal mucosa is free and firm . • In an enlarged prostate , in case of carcinoma prostate , the mucosa of the rectum cannot be moved, if there is infiltration into rectum. • GRADING OF PROSTATE ( Roger Barnes grading ) I. Prostatic lobes protrude minimally into the rectal lumen by 1-2 cm and median sulcus is palpable. II. Prostatic lobes protrude 2-3 cm into the rectal lumen and the median sulcus is obliterated. III. Prostatic lobes protrude 3-4 cm into the rectal lumen. IV. Prostatic lobes protrude >4 cm & most of the rectal lumen is filled by the projecting prostatic lobes .
- 20. INVESTIGATIONS: • ESSENTIAL investigations ■ Urine analysis by dipstick for blood, glucose and protein ■ Urine culture for infection ■ Serum creatinine ■ Urinary flow rate and residual volume measurement • ADDITIONAL investigations ■ PSA if indicated ■ Pressure–flow studies
- 21. • BLOOD UREA & CREATININE : Raised level indicate renal failure • UROFLOWMETRY: The person is asked to void urine from their full bladder into the flowmeter . The flow rate is assessed. PEAK FLOW RATE – Normal peak flow rate : > 15 ml/sec Doubtful peak obstruction : 10-15 ml/sec Definite peak obstruction : < 10 ml/sec Thus , the degree of bladder outlet obstruction can be secured by uroflowmetry. • ULTRASONOGRAM : To assess the size and weight of the prostate , assess the residual urine , and look for hydroureteronephrosis & bladder wall changes.
- 23. •URODYNAMIC STUDIES: They should be performed on the following patients: • men with suspected neuropathy (Parkinson’s disease, dementia, longstanding diabetes, previous strokes, multiple sclerosis); • men with a dominant history of irritative symptoms and men with lifelong urgency and frequency; • men with a doubtful history and those with flow rates in the near normal range (~ or > 15 ml s–1); • men with invalid flow rate measurements (because of low voided volumes)
- 26. MEDICAL TREATMENT: • ALPHA- ADRENERGIC BLOCKERS : inhibit the contraction of smooth muscle that is found in the prostate and relax the internal sphincter for better bladder drainage . Given as monotherapy when the prostate is <40g as measured by ultrasound. Eg : TAMSULOSIN (Most selective) , TERAZOSIN , ALFAZOSIN. Latest drug : SILODOSIN 4-8 mg once nightly. • 5-ALPHA REDUCTASE INHIBITOR : which inhibit the conversion of testosterone to DHT, the most active form of androgen. Eg: FINASTERIDE ACETATE 5mg daily for 6 months . Helps in preventing hyperplasia of prostate. Given in case of large prostates . Other drug: DUTASTERIDE 0.5mg once daily for 6-12 months.
- 27. SURGICAL TREATMENT: INDICATIONS • 1 Acute retention : in fit men with no other cause for retention (drugs, constipation, recent operation, etc.) (accounts for 25% of prostatectomies) • 2 Chronic retention and renal impairment: a residual urine of 200 ml or more, a raised blood urea, hydroureter or hydronephrosis demonstrated on urography and uraemic manifestations (accounts for 15% of prostatectomies). • 3 Complications of bladder outflow obstruction: stone, infection and diverticulum formation.
- 28. • 4 Haemorrhage: occasionally, venous bleeding from a ruptured vein overlying the prostate will require prostatectomy to be performed. • 5 Elective prostatectomy for severe symptoms: this accounts for about 60% of prostatectomies. Increasing difficulty in micturition, with considerable frequency day and night, delay in starting and a poor stream are the usual symptoms for which prostatectomy is advised. CONTD
- 29. TRANSURETHRAL RESECTION OF PROSTATE (TURP): • GOLD STANDARD method of surgery. • A rectoscope is passed through the urethra , and under vision with constant irrigation with water or 1.5 percent glycerine , prostate is resected into multiple pieces and removed. • Haemostasis is obtained by cauterization. COMPLICATIONS OF TURP: • TURP Syndrome : nausea , confusion, vomiting , visual disturbances. • Retrograde ejaculation (15%) • Impotence (5-10%) • Incontinence (<1%) • Bladder neck contracture.
- 30. TRANSVESICAL SUPRAPUBIC PROSTATECTOMY(FRAYERS) • EXTRAPERITONEAL APPROACH: bladder is opened , prostate is enucleated with a finger & bleeding is controlled by inflating the foleys bulb with 30-50 ml of air and by ligatures. • Bladder is drained by a Malecots catheter , which is wider than foleys catheter , it can drain potential bleeding in the bladder. • During the process, prostatic urethra is also avulsed. • After about 7-10 days a tract develop along the length of foley catheter , heals by granulation and fibrosis , form a future prostatic urethra.
- 31. This method is now restricted to glands >100g in weight associated with calculus. And in orthopaedic condition like ankylosis of hip ( difficulty in positioning) DISADVANTAGES: • Blind resection • Increased risk of haemorrhage • Stricture of prostatic urethra.
- 32. RETROPUBIC PROSTATECTOMY • Performed by an extraperitoneal approach without opening the bladder by pushing the bladder to one side and excising the prostate . NEWER TREATMENTS: • Holmium:YAG laser: for >100g prostate patients. • Intraurethral stents: who are grossly unfit for surgery.
- 33. COMPLICATIONS : AFTER TREATMENT • Haemorrhage Water intoxication (fluid excess) • Sepsis Osteitis pubis • Incontinence Cardiovascular • Retrograde ejaculation • Impotence Myocardial infarction • Stricture Pulmonary atelectasis Pneumonia CCF DVT local General
- 34. COUNSELLING OF PATIENTS • Retrograde ejaculation - 65% of men after prostatectomy. • Erectile impotence- This occurs in about 5% of men. • The risk of reoperation- After TURP, this is about 15% after 8–10 years.