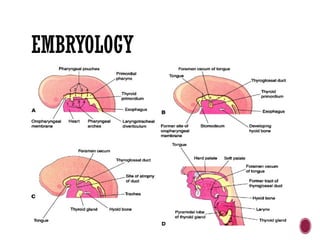
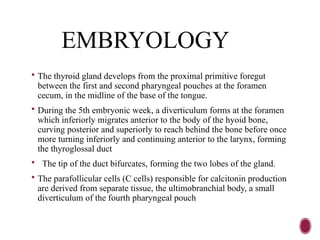
EMBRYOLOGY
The thyroidgland develops from the proximal primitive foregut
between the first and second pharyngeal pouches at the foramen
cecum, in the midline of the base of the tongue.
During the 5th embryonic week, a diverticulum forms at the foramen
which inferiorly migrates anterior to the body of the hyoid bone,
curving posterior and superiorly to reach behind the bone before once
more turning inferiorly and continuing anterior to the larynx, forming
the thyroglossal duct
The tip of the duct bifurcates, forming the two lobes of the gland.
The parafollicular cells (C cells) responsible for calcitonin production
are derived from separate tissue, the ultimobranchial body, a small
diverticulum of the fourth pharyngeal pouch
5.
ANATOMY OF THETHYROID GLAND
The thyroid gland develops within the third week of gestation. In the
embryo, the thyroid begins its initial development at the base of the
tongue. It descends down the thyroglossal duct to ultimately rest anterior
to the trachea.
It is fully functional by the end of the first trimester.
The thyroid extends from C5 to T1 and lies anterior to the thyroid and
cricoid cartilages of the larynx and the first five or six tracheal rings.
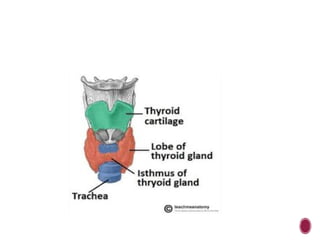
The thyroid consists of a right and a left lobe. A bridge of tissue, the
isthmus, crosses over the midline of the neck anterior to the trachea,
providing a link between the two thyroid lobes.
Occasionally, individuals may have a superior extension of the isthmus.
This normal variant is termed a pyramidal lobe. Agenesis of a lobe may
also occur.
7.
PHSIOLOGY OF THETHYROID GLAND
The hypothalamus, located within the brain, produces thyroid-releasing
hormone, which in turn controls the release of thyroid-stimulating
hormone (TSH) by the anterior pituitary gland.
As a result of the TSH released by the pituitary gland, the thyroid, in turn,
releases the hormones contained within its cells. These hormones are
thyroxine (T4), triiodothyronine (T3), and calcitonin .
The thyroid utilizes iodine to manufacture its hormones. Iodine is found in
some vegetables, seafood, and within many processed foods that contain
iodized salt. Accordingly, the subscripted numbers “3” and “4” found in the
thyroid hormones denote the number of iodine atoms contained within each
hormone.
8.
Thyroxine isthe most abundant hormone produced by the thyroid
however, each hormone is vital, and they work together to regulate
metabolism, growth and development, and the activity of the nervous
system.
A surplus of these hormones will produce hyperthyroidism and a
reduction will cause hypothyroidism.
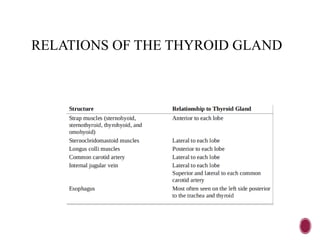
ANATOMY
Arterial supply
superior thyroid artery (from the external carotid artery)
inferior thyroid artery (from the thyrocervical trunk)
if the inferior thyroid artery arises from the subclavian artery
it is referred to as an accessory inferior thyroid artery
Venous drainage
superior thyroid vein(drains to the internal jugular vein)
middle thyroid vein (drains to the internal jugular vein)
inferior thyroid vein (drains via plexus to the brachiocephalic
vein)
12.
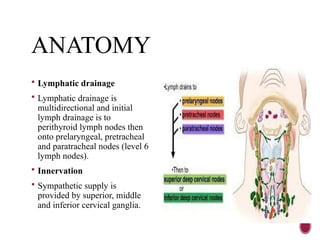
ANATOMY
Lymphatic drainage
Lymphatic drainage is
multidirectional and initial
lymph drainage is to
perithyroid lymph nodes then
onto prelaryngeal, pretracheal
and paratracheal nodes (level 6
lymph nodes).
Innervation
Sympathetic supply is
provided by superior, middle
and inferior cervical ganglia.
INDICATION FOR THYROIDU/S
palpable mass found within the neck.
abnormal laboratory findings.
a follow-up examination from nuclear medicine studies and other
diagnostic imaging studies.
Preoperative determination of the extent of known thyroid
malignancy
Detection of residual ,recurrent or metastatic carcinoma
Guidance to FNAB for non-palpable nodules
15.
TECHNIQUE
Expose thelower neck and protect the clothes below the neck from
gel, remove jewelry.
superficial probe-high frequency(linear) 7-14MHZ.
-use curvilinear(3.5-5Mhz) for gross enlargement and in obese patients.
cervical spine/neck extended; you may support with apillow.
start with atransverse along the midline superior to inferior.
then scan longitudinal from the lateral to right lateral while tilting the
head away towards the contra-lateral side.
survey adjacent structures for enlarged lymphnodes(especially in the
level 6 for cervical lymphnodes,pre-and para tracheal, peri thyroid
and pre laryngeal nodes) or other pathology in the adjacent muscles or
vascular bundle.
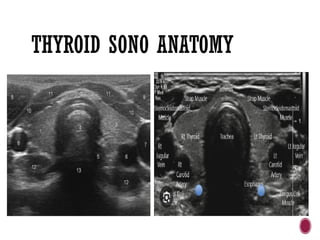
SONOGRAPHIC ANATOMY.
Normalthyroid tissue is homogenous and consists of medium- to
high-level echogenicities similar to that of the testes surrounded by
athin hyperechoic line.
Each adult pear-shaped lobe measures approximately 4 to 6 cm in
length, 2 to 3 cm in width, and 1 to 2 cm in thickness, with the right
lobe typically being the largest.
The isthmus normally measures between 2 or 4 to 6 mm in the
anteroposterior dimension.
A sonographic examination of the entire neck should also be
performed for enlarged lymph nodes or masses.
18.
There areseveral prominent muscles and vascular structures that delineate the
margins of the thyroid gland . The neck muscles, which appear more hypoechoic
than the normal thyroid tissue, are easily seen with sonography. The thin
infrahyoid or strap muscles, which include the sternohyoid, sternothyroid,
thyrohyoid, and omohyoid, are found anterior to the thyroid gland.
The much larger sternocleidomastoid muscles pass lateral to the thyroid lobes.
The longus colli muscles are seen posterior to each lobe.
The common carotid artery and internal jugular vein will be seen lateral to each
lobe as anechoic tubes in the longitudinal plane and circles in the transverse
plane.
The esophagus lies posterior to the thyroid gland, mostoften on the left side, and
can often resemble a mass. To differentiate the esophagus from a mass, one can
have the patient swallow. Upon real-time observation of swallowing, the saliva
can be visualized passing through the esophagus.
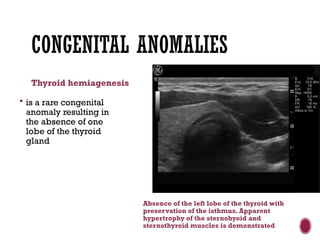
CONGENITAL ANOMALIES
Thyroid hemiagenesis
is a rare congenital
anomaly resulting in
the absence of one
lobe of the thyroid
gland
Absence of the left lobe of the thyroid with
preservation of the isthmus. Apparent
hypertrophy of the sternohyoid and
sternothyroid muscles is demonstrated
21.
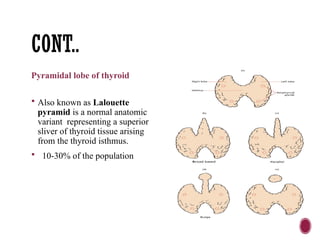
CONT..
Pyramidal lobe ofthyroid
Also known as Lalouette
pyramid is a normal anatomic
variant representing a superior
sliver of thyroid tissue arising
from the thyroid isthmus.
10-30% of the population
22.
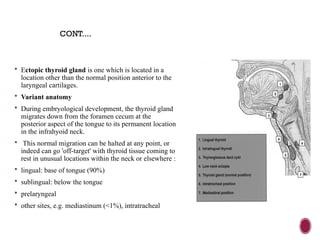
Ectopic thyroidgland is one which is located in a
location other than the normal position anterior to the
laryngeal cartilages.
Variant anatomy
During embryological development, the thyroid gland
migrates down from the foramen cecum at the
posterior aspect of the tongue to its permanent location
in the infrahyoid neck.
This normal migration can be halted at any point, or
indeed can go 'off-target' with thyroid tissue coming to
rest in unusual locations within the neck or elsewhere :
lingual: base of tongue (90%)
sublingual: below the tongue
prelaryngeal
other sites, e.g. mediastinum (<1%), intratracheal
CONT....
23.
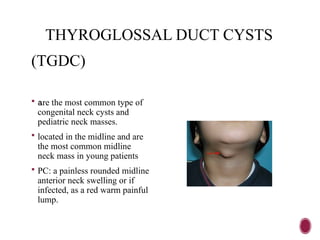
THYROGLOSSAL DUCT CYSTS
(TGDC)
are the most common type of
congenital neck cysts and
pediatric neck masses.
located in the midline and are
the most common midline
neck mass in young patients
PC: a painless rounded midline
anterior neck swelling or if
infected, as a red warm painful
lump.
24.
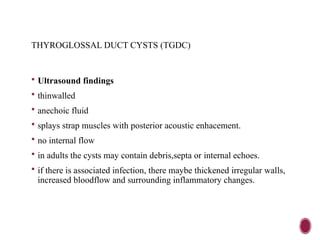
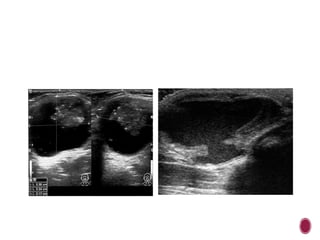
THYROGLOSSAL DUCT CYSTS(TGDC)
Ultrasound findings
thinwalled
anechoic fluid
splays strap muscles with posterior acoustic enhacement.
no internal flow
in adults the cysts may contain debris,septa or internal echoes.
if there is associated infection, there maybe thickened irregular walls,
increased bloodflow and surrounding inflammatory changes.
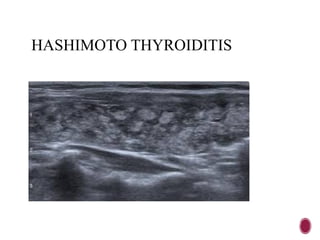
HASHIMOTO THYROIDITIS AND
HYPOTHYROIDISM
Hypothyroidism is a condition that results from the underproduction of thyroid
hormones. Hashimoto thyroiditis is an autoimmune disease, which is the most
common cause of hypothyroidism in the United States.
In Hashimoto disease, the thyroid becomes inflamed, and, as a result, the thyroid
produces smaller amounts of thyroid hormones. In order to compensate, the pituitary
gland releases more TSH, which causes the thyroid to become enlarged.
Clinically, many patients are asymptomatic in the earlystages of the disease.
However, as the disease progresses, they may present with puffiness under the eyes,
puffy face, dry skin, slight weight gain, depression, increased cold sensitivity, and
elevated blood cholesterol levels
The end-stage of the disease may actually lead to fibrosis and atrophy of the gland.
Sonographically, the thyroid will appear, diffusely heterogeneous, coarse, and mildly
enlarged with increased vascularity within the gland
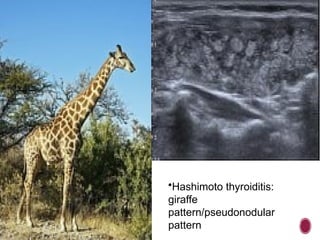
Oftentimes, multiple, ill-defined hypoechoic regions separated by fibrous
hyperechoic tissue will be demonstrated with Hashimoto thyroiditis.
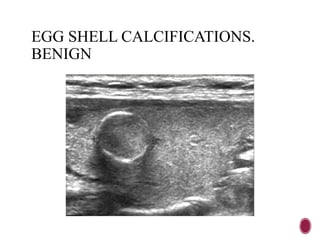
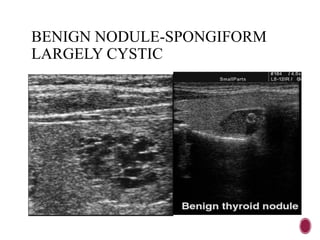
BENIGN THYROID NODULES
. Benign thyroid nodules are the most common masses identified within the thyroid
gland with sonography.
sonographic appearances including completely anechoic, isoechoic, or hyperechoic ,
wider than tall, no local tissue invasion, egg shell calcifications and well marginated
borders. They may also have a surrounding halo and acomet tail or ringdown artifact.
Nodular hyperplasia is the most common cause of thyroid nodules.
There are different types of thyroid nodules.
Colloid nodules. These are one or more overgrowths of normal thyroid tissue. These
growths are not cancerous (benign), may grow large, but do not spread beyond the
thyroid gland.
Thyroid cysts. These are fluid-filled or partially solid/partially fluid-filled growths
inside the thyroid gland.
36.
THYROID NODULES
Inflammatorynodules. These nodules develop as a result of
chronic inflammation of the thyroid gland. These growths may or
may not cause pain.
Multinodular goiter. Sometimes an enlarged thyroid (goiter) is
composed of many, usually benign, nodules.
Hyperfunctioning thyroid nodules. These nodules produce
thyroid hormone, which may lead to the development of
hyperthyroidism.
Thyroid cancer. Of the nodules that can form as the thyroid gland
enlarges, fortunately, less than 5 percent are cancerous.
37.
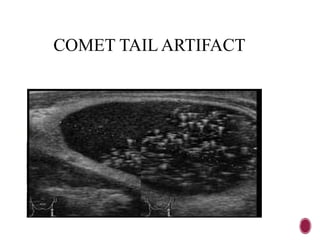
COLLOID NODULES
Pathology
Colloid nodules are composed of irregularly enlarged follicles containing
abundant colloid.
Some colloid nodules can be cystic (cystic colloid nodule) and may contain
areas of necrosis, hemorrhage and/or calcification.
Ultrasound
iso- to hypoechoic
may have internal cystic or heterogeneous change
may have calcification
multiple echogenic foci (of inspissated colloid) with comet tail artifact
38.
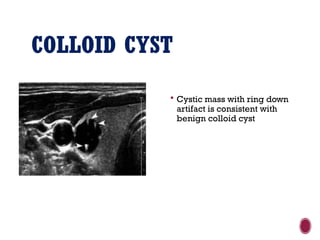
COLLOID CYST
Cysticmass with ring down
artifact is consistent with
benign colloid cyst
39.
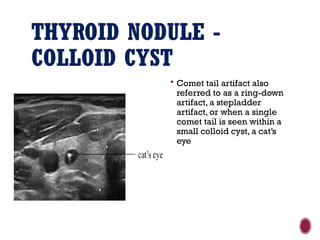
THYROID NODULE -
COLLOIDCYST
Comet tail artifact also
referred to as a ring-down
artifact, a stepladder
artifact, or when a single
comet tail is seen within a
small colloid cyst, a cat’s
eye
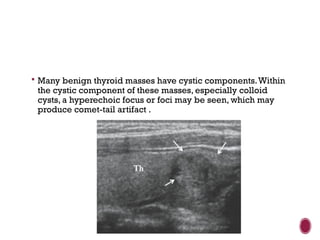
Many benignthyroid masses have cystic components.Within
the cystic component of these masses, especially colloid
cysts, a hyperechoic focus or foci may be seen, which may
produce comet-tail artifact .
44.
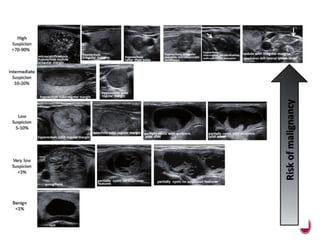
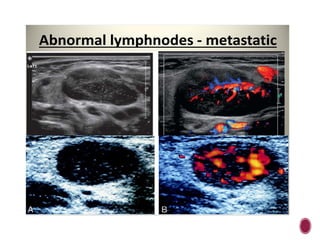
MALIGNANT THYROID NODULES.
Hypoechoic or hperechoic mass
Taller-than-wide shape
micro-calcifications especially intranodular rather than periphery.
Solitary mass
Marked vascularity within the central part of the nodule
irregular surrounding halo.
Extracapsular invasion
Lobulated margins
Enlargement of the cervical lymph nodes (metastasis)
45.
THYROID MALIGNANCIES
PRIMARY
-papillary-78%, some are mixed(papillary-follicular)
-follicular-17%
-medullary-4%
anaplastic-1%
SECONDARY( VERY RARE)
-Lymphoma
-metastases
48.
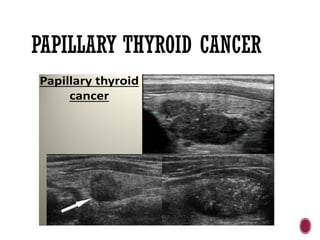
PAPILLARY THYROID CARCINOMA
Papillary thyroid carcinoma (PTC) is the most common malignancy of
the thyroid gland .
Presentation is usually with a solitary palpable thyroid mass.
Papillary carcinoma has a tendency to metastasize early to local lymph
nodes, with 50% of patients having nodal involvement at presentation
ultrasound features.
solitary mass usually with an irregular outline, located in the subcapsular
region and demonstrating vascularity
microcalcifications may be present .
Lymph node metastases have a tendency to completely cavitate
They tend to have septations, mural nodules and relatively thick walls
49.
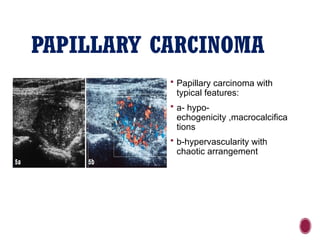
PAPILLARY CARCINOMA
Papillarycarcinoma with
typical features:
a- hypo-
echogenicity ,macrocalcifica
tions
b-hypervascularity with
chaotic arrangement
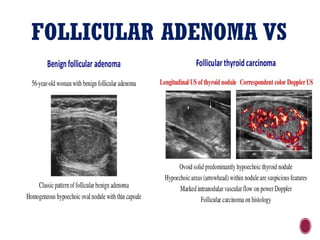
FOLLICULAR THYROID ADENOMA
Follicular thyroid adenoma is a commonly found benign neoplasm
of the thyroid .
Macroscopically follicular adenomas are round to oval, with a
surrounding fibrous capsule that is usually regular and thin. They
typically range in size between 1 and 3 cm, and changes including
cystic degeneration, hemorrhage, ossification, calcification and
fibrosis can be seen
52.
FOLLICULAR THYROID
ADENOMA
Ultrasound
Ultrasound features of follicular adenomas share many features with
follicular carcinomas. In general follicular thyroid adenomas:
thin peripheral halo
predominantly cystic or mixed cystic and solid lesions
isoechoic or predominantly anechoic
can be homogenous or heterogeneous
absence of internal flow or predominantly peripheral flow indicates is
associated with reduced probability of thyroid follicular malignancy
53.
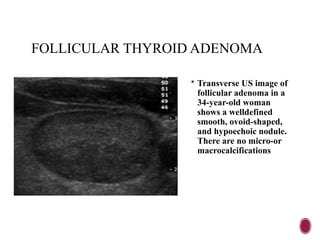
FOLLICULAR THYROID ADENOMA
Transverse US image of
follicular adenoma in a
34-year-old woman
shows a welldefined
smooth, ovoid-shaped,
and hypoechoic nodule.
There are no micro-or
macrocalcifications
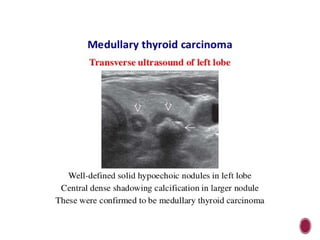
MEDULLARY THYROID CARCINOMA
(MTC)
Medullary thyroid carcinoma (MTC) is a subtype of
thyroid cancer which accounts for 5-10% of all thyroid
malignancies.
Ultrasound
Punctate high echogenic foci resembling calcification may
be seen both within the primary thyroid lesion as well as
metastatic regional lymph nodes and distant metastatic
sites.
Involved lymph nodes typically calcify
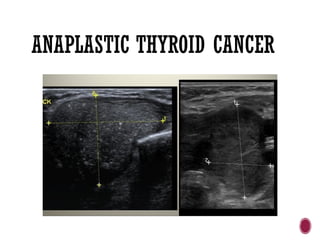
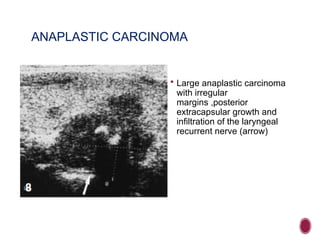
ANAPLASTIC CARCINOMA
Largeanaplastic carcinoma
with irregular
margins ,posterior
extracapsular growth and
infiltration of the laryngeal
recurrent nerve (arrow)
62.
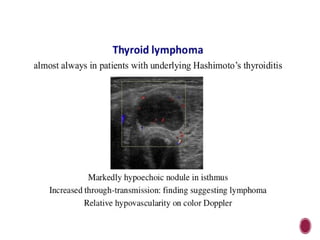
THYROID LYMPHOMA
Uncommon:< 5% of all thyroid malignancies
Almost always in patients with underlying Hashimoto’s thyroiditis
Classically presents with rapidly enlarging thyroid gland
Ultrasound features: Markedly hypoechoic nodule in background of
chronic thyroiditis Enhanced through transmission posterior to the
lesion
Treatment: Chemotherapy and external beam radiation Surgery only
if trachea markedly compressed by tumor
Good prognosis when disease confined to thyroid gland
64.
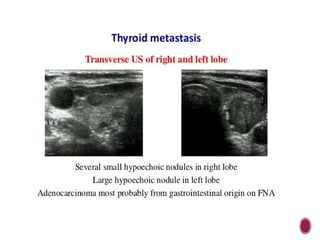
THYROID METASTASIS
Thyroidmetastasis rare in daily clinical practice
Generally associated with advanced stage of malignancy
Main primary tumors spreading to thyroid gland: malignant
melanoma, breast carcinoma, renal cell carcinoma
Difficult to distinguish from primary thyroid lesion
No specific features on US: Solitary/multiple hypoechoic nodules
without calcifications No specific information about color Doppler of
metastases
66.
GOITER.
A goiteris defined as an enlarged, hyperplastic thyroid gland. It has
many causes, including iodine deficiency, Graves disease, and
thyroiditis.
Clinically, patients with a goiter often have a palpable (and often
visually) enlarged thyroid gland. The enlarged gland can cause a
feeling of tightening in the throat, dysphagia, dyspnea, coughing, and
hoarseness.
Sonographically,
the thyroid will appear enlarged and heterogeneous.
The enlarged thyroid gland that contains multiple nodule with cystic
and solid components may be referred to as a multinodular goiter or
adenomatous goiter.
67.
GRAVES DISEASE ANDHYPERTHYRODISM
CLINICAL FINDINGS OF GRAVES
DISEASE
1. Bulging eyes
2. Heat intolerance
3. Nervousness
4. Weight loss
5. Hair loss
SONOGRAPHIC FINDINGS OF
GRAVES DISEASE
1. Enlarged gland
2. Heterogeneous or diffusely
hypoechoic echotexture
3. Thyroid inferno(increased vascularity)
68.
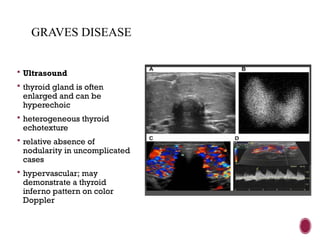
GRAVES DISEASE
Ultrasound
thyroid gland is often
enlarged and can be
hyperechoic
heterogeneous thyroid
echotexture
relative absence of
nodularity in uncomplicated
cases
hypervascular; may
demonstrate a thyroid
inferno pattern on color
Doppler
69.
DE QUERVAIN THYROIDITIS
OR subacute granulomatous thyroiditis, is a form of self-limited
subacute thyroiditis usually preceded by an upper respiratory tract
viral infection such as mumps, measles, coxsackie virus, adenovirus,
and influenza viruses.
Epidemiology
It usually affects middle-aged females( 2nd-5th decades of life).
Clinical presentation
Most patients present with a painful neck , low grade fever and
occasional dysphagia.
70.
DE QUERVAIN THYROIDITIS
Ultrasound
The most commonly described sonographic appearance is poorly
defined regions of decreased echogenicity with decreased vascularity
in the affected areas .
These can be bilateral or unilateral.
The thyroid gland size is mostly normal but can occasionally be
enlarged or smaller in size
71.
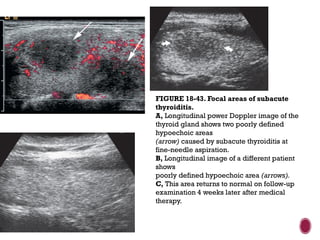
FIGURE 18-43. Focalareas of subacute
thyroiditis.
A, Longitudinal power Doppler image of the
thyroid gland shows two poorly defined
hypoechoic areas
(arrow) caused by subacute thyroiditis at
fine-needle aspiration.
B, Longitudinal image of a different patient
shows
poorly defined hypoechoic area (arrows).
C, This area returns to normal on follow-up
examination 4 weeks later after medical
therapy.
#3 it is the first gland to develop in the embryo, it starts to develop around the 24th day and begins to function around the 12th week. it arises from the first and second pharyngeal pouches. it is endodermal in origin.
there is formation of the thyroid primordium, and thereafter there is formation of the diverticulum to form the duct known as the thyroglossal duct. the upper part of its invagination is known as the foramen cecum.
this duct crosses the midline structures like thepharyngeal part of the gut,developing hyoid bone .and laryngeal cartilages. the lower end of the duct bifurcates forming the right and left lobes along with the isthmus and by end of the 7th week it achieves its ultimate position
fate of the thyroglossal duct.
it degenarates but stays in some percentage of people forming the pyramidal lobe.
#18 Each thyroid lobe should be evaluated using color Doppler because increase vascularity or hyperemia may be evident with Graves disease and Hashimoto thyroiditis
#22 LINGUAL-FAILED MIGRATION /INCOMPLETE DESCENT OF THE THYROID. SUBLINGUAL-RESULTS FROM INCOMPLETE DESCENT OF THE THYROID
#23 it results from abuild up of secretions with in the duct. the cyst can become infected to form afistula which discharges onto the skin of the anterior neck.
#25 Ultrasound of the neck detected a supralaryngeal cyst in size of 2.30 Â 2.24 Â 2.17 cm above the hyoid bone, including solid tissue within the cyst.
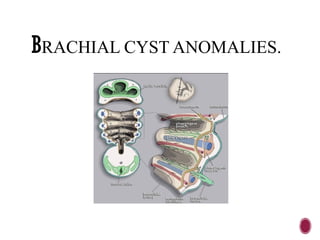
#26 he anomalies result from branchial apparatus (six arches; five clefts), which are the embryologic precursors of the ear and the muscles, blood vessels, bones, cartilage, and mucosal lining of the face, neck, and pharynx 1.
During the 3rd to 5th week of embryonic development, the second arch grows caudally and covers the third, fourth and sixth arches. When it fuses to the skin caudal to these arches, the cervical sinus is formed. Eventually, the edges of cervical sinus fuse and the ectoderm within the tube disappears 9. Persistence of branchial cleft or pouch results in a cervical anomaly located along the anterior border of the sternocleidomastoid muscle from the tragus of the ear to the clavicle 10








![Thyroid_Gland_Introduction&embryology[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidglandintroductionembryology1-250604192159-6ad15b98-thumbnail.jpg?width=640&height=640&fit=bounds)










































![carotid stenosis [Autosaved].pptx for master students](https://cdn.slidesharecdn.com/ss_thumbnails/carotidstenosisautosaved-241229032708-f20dd02c-thumbnail.jpg?width=640&height=640&fit=bounds)




















