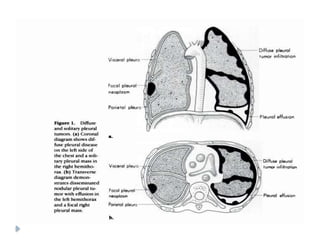
• The pleurais a thin, smooth,
glistening, delicate serous
membrane which
1. Covers the lungs
2. Lines the wall of the thorax
3. This is a layer of
mesothelial cells, supported
by connective tissue.
5.
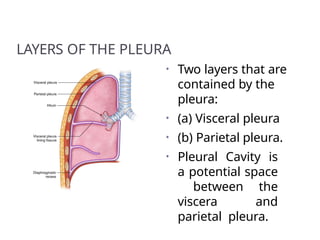
LAYERS OF THEPLEURA
• Two layers that are
contained by the
pleura:
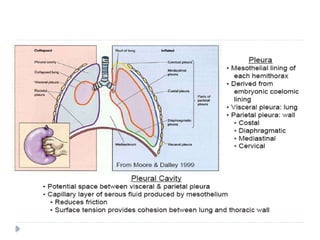
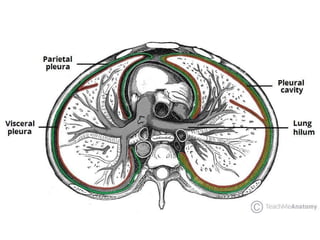
• (a) Visceral pleura
• (b) Parietal pleura.
• Pleural Cavity is
a potential space
between the
viscera and
parietal pleura.
6.
Structure of thePleurae
• Each pleura can be divided into two
parts:
• Parietal pleura – covers the internal
surface of the thoracic cavity.
• Visceral Pleura
• Covers the lungs.
• The visceral pleura covers the outer
surface of the lungs, and extends into
the interlobar fissures.
7.
Parietal Pleura
• Theparietal pleura covers the internal
surface of the thoracic cavity.
• It is thicker than the visceral pleura
• can be subdivided according to the part
of the body that it is contact with:.
1. Costal pleura.
2. Diaphragmatic pleura.
3. Mediastinal pleura.
4. Cervical pleura.
8.
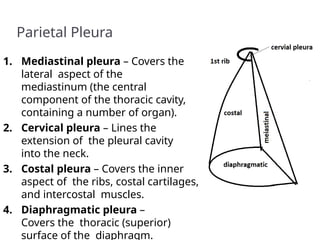
Parietal Pleura
1. Mediastinalpleura – Covers the
lateral aspect of the
mediastinum (the central
component of the thoracic cavity,
containing a number of organ).
2. Cervical pleura – Lines the
extension of the pleural cavity
into the neck.
3. Costal pleura – Covers the inner
aspect of the ribs, costal cartilages,
and intercostal muscles.
4. Diaphragmatic pleura –
Covers the thoracic (superior)
surface of the diaphragm.
9.
VISCERAL PLEURA (PULMONARY
PLEURA)
•The visceral pleura entirely covers the
top layer of the lung with the
exception of at the hilum and along
the connection of the pulmonary
ligament.
• It also extends in the depths of the
fissures of the lungs.
• It is firmly adherent to the lung
surface and can’t be divided from it.
11.
Pleural Cavity
• Thepleural cavity is a potential space
between the parietal and visceral pleura. It
contains a small volume of serous fluid,
which has two major functions.
• It lubricates the surfaces of the pleurae,
allowing them to slide over each other.
• The serous fluid also produces a surface
tension, pulling the parietal and visceral
pleura together.
• This ensures that when the thorax
13.
Pleural Recesses
• Anteriorlyand posteroinferiorly, the pleural cavity is not
completely filled by the lungs. This gives rise
to recesses – where the opposing surfaces of the
parietal pleura touch.
• There are two recesses present in each pleural cavity:
• Costodiaphragmatic – located between the costal
pleurae and the diaphragmatic pleura.
• Costomediastinal – located between the costal pleurae
and the mediastinal pleurae, behind the sternum.
– These recesses are of clinical importance, as they
provide a location where fluid can collect (such as in a
pleural effusion).
15.
Pleural fluid
Thepleural space contains a tiny amount of fluid
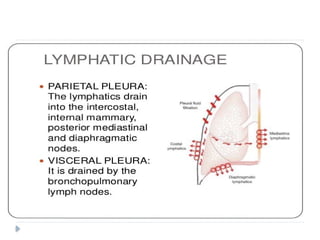
Pleural fluid is produced at parietal level ,mainly in
less dependant regions of the cavity .
Reabsorption is accomplished by parietalpleural
lymphatics in the most dependent part of the cavity
on the diaphragmatic surface and mediatinalregions .
The flow rate in pleural lymphatics can increase in
response to an increase in pleural fluid filtration .
(negative feedback mechanism )
When filtration exceeds maximum pleural lypmhatic
flow pleural effusions occur .
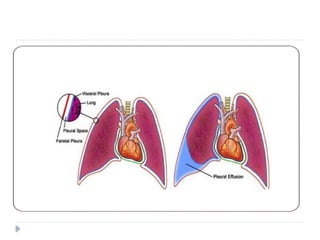
A pleuraleffusion is a pathologic fluid collection within the
pleural cavity.
Normally 10 15 mL of fluid is present and this serves as a
−
lubricant between the parietal and visceral pleural layers.
Pleural effusions may reach volumes of up to a few liters and
these large effusions result in compression of the underlying
lung, contralateral displacement of the mediastinum, and
depression of the hemidiaphragm
Pleural effusions develop when there is excess pleural fluid
produced, diminished resorption of fluid from the pleural
space, or both.
The fluid can originate from the pleura or be extra pleural in
origin
NOTE : The role of imaging asses the cause of the effusion .
Pathology
Pleural effusionsmay be classified according to their
composition:
Pleural transudate:
Clear fluid with a specific gravity of less than 1.016 and a
protein content of less than 3 g/dL.
The Pandy test is negative.
Left ventricular failure is the most common cause of a
transudate.
Ascites in hepatic cirrhosis, nephrotic syndrome, and
myxedema may also cause transudative effusions.
22.
Pleural exudate:
An opaque fluid with a protein content of more than
3 g/dL, a specific gravity of greater than 1.016,
There is positive Pandy test.
The microscopic identification of cellular elements
such as granulocytes, lymphocytes, erythrocytes, and
malignant cells narrows the differential diagnosis.
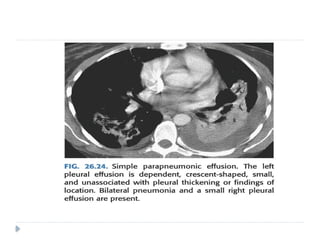
Parapneumonic effusions are most common and are
usually secondary to pulmonary infections.
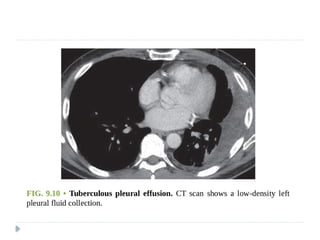
Tuberculous exudate is distinguished by its high
lymphocyte content.
Malignant pleural effusions are also exudates
although malignant cells may not always be detected
on cytologic evaluation.
23.
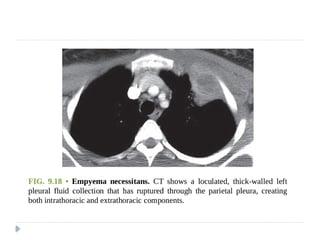
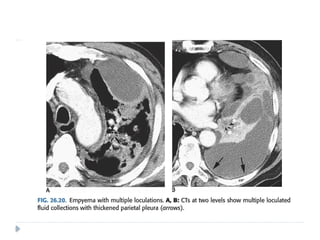
Empyema:
Ispus in the pleural cavity.
The diagnosis is made when the pleural fluid is obviously purulent
when organisms are identified in the fluid, or when the fluid has an
elevated white blood cell count
is usually either parapneumonic or postpneumonic.
Less commonly it may result from transdiaphragmatic extension of
a liver abscess.
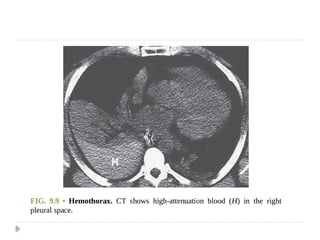
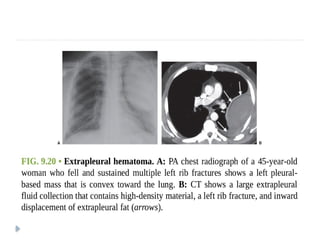
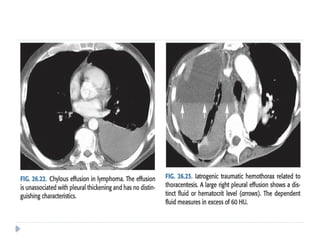
Hemothorax:
Bleeding into the pleural space
may be secondary to trauma, aortic rupture, or pleural malignancy.
Occasionally, it is seen in thromboembolic disease when
complicated by pulmonary infarction.
27.
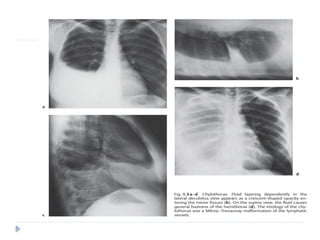
Chylothorax:
Achylothorax contains fluid that is largely chyle (lymph of
intestinal origin).
Because chyle usually contains suspended fat in the form of
chylomicrons, chylothorax fluid may be milky.
Three main mechanisms account for chyle collections in the
pleural space: (i) leakage from a discrete rupture of the thoracic
duct or a large lymphatic vessel
(ii) a general oozing from pleural lymphatics,
(iii) passage of chylous ascites through the diaphragm
Approximately 50% of chylothoraces are of neoplastic origin
25% are traumatic,
15% are idiopathic
Lymphomas make up about 75% of the neoplastic lesions , and
chylothorax can be the initial feature of lymphomas
29.
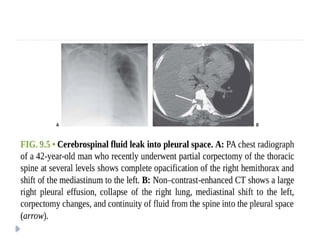
Bilious andcerebrospinal fluid (CSF) pleural
effusions:
Both are extremely rare.
Bilious effusions are seen posthepatic and after
diaphragmatic lacerations.
A traumatic fistula to the spinal subarachnoid
space allows CSF to enter the pleural space
31.
Clinical Features;
1.Symptoms most often due to underlying
disease process
2. Small pleural effusions – often asymptomatic
3. New effusion – often localized pain or
referral to shoulder
4. Large effusion (> 500 ml) dyspnea on
exertion or rest
5. Acute pleuritic pain – think pleurisy or
pulmonary infarction
32.
Radiologic Findings
ChestRadiograph
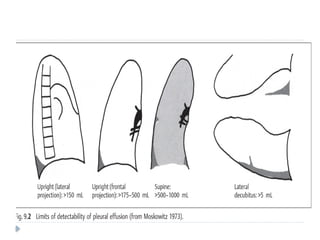
Upright position:
The lateral chest radiograph shows homogeneous
opacification of the posterior costophrenic angle
with a superiorly concave meniscus.
The Posteroanterior (PA) chest radiograph shows
obliteration of the costophrenic and cardiophrenic
angles if the effusion is greater than approximately
175 mL The meniscus is concave toward the lung
and becomes thinner superiorly.
33.
Supine position:
Effusions are only visible on supine radiographs
when they exceed 500 mL
Manifestations include:
1. The diaphragmatic contour is obscured
2. Opacification of the lateral costophrenic angles
3. Generalized “haziness” of the hemithorax
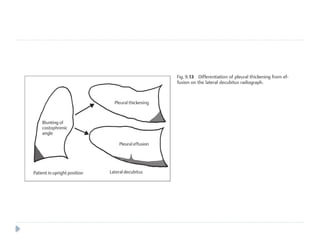
Lateral decubitus position:
Fluid collects between the lateral chest wall and
the lung, producing a band of opacification
which may enter the minor fissure.
36.
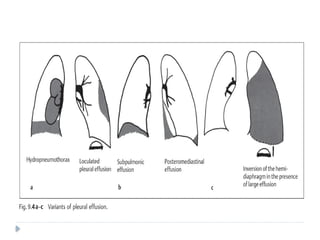
Atypical forms ofpleural effusion
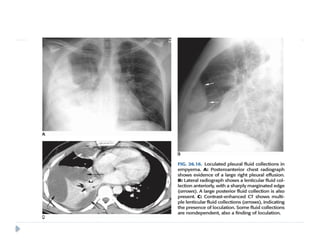
Loculated effusion:
Adhesions between the visceral and parietal
pleura result in development of loculated
collections along the inner aspect of the chest
wall.
En face, they may appear as ill-defined round
opacities but tangentially they produce a
semicircular opacity whose margins form an
obtuse angle with the chest wall.
This helps to distinguish them from peripheral
pulmonary tumors, which usually form an acute
37.
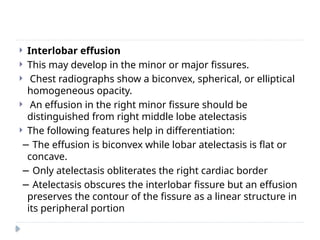
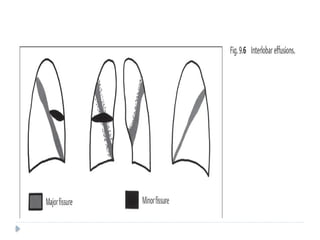
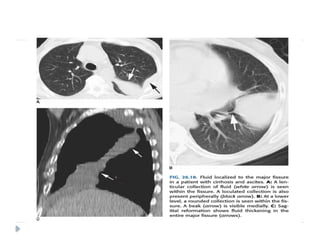
Interlobar effusion
This may develop in the minor or major fissures.
Chest radiographs show a biconvex, spherical, or elliptical
homogeneous opacity.
An effusion in the right minor fissure should be
distinguished from right middle lobe atelectasis
The following features help in differentiation:
− The effusion is biconvex while lobar atelectasis is flat or
concave.
− Only atelectasis obliterates the right cardiac border
− Atelectasis obscures the interlobar fissure but an effusion
preserves the contour of the fissure as a linear structure in
its peripheral portion
42.
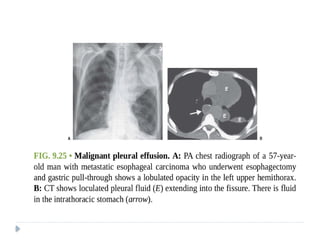
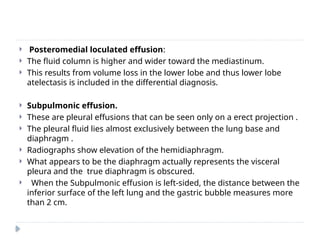
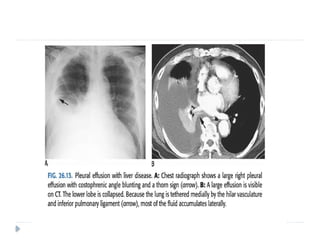
Posteromedial loculatedeffusion:
The fluid column is higher and wider toward the mediastinum.
This results from volume loss in the lower lobe and thus lower lobe
atelectasis is included in the differential diagnosis.
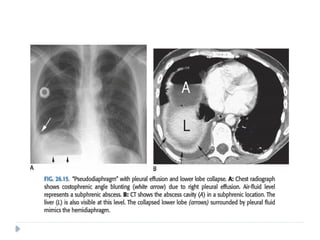
Subpulmonic effusion.
These are pleural effusions that can be seen only on a erect projection .
The pleural fluid lies almost exclusively between the lung base and
diaphragm .
Radiographs show elevation of the hemidiaphragm.
What appears to be the diaphragm actually represents the visceral
pleura and the true diaphragm is obscured.
When the Subpulmonic effusion is left-sided, the distance between the
inferior surface of the left lung and the gastric bubble measures more
than 2 cm.
44.
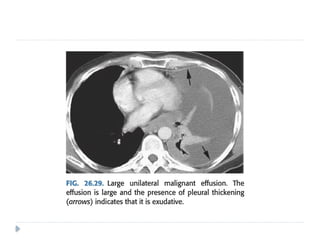
CT scanningis excellent at detecting small amounts of
fluid and is also often able to identify the underlying
intrathoracic causes (e.g. malignant pleural deposits or
primary lung neoplasms) as well as subdiaphragmatic
diseases (e.g. subdiaphragmatic abscess).
CT is not able to differentiate between a transudative
or exudative pleural effusion with similar fluid densities
and non-differentiating rates of loculation and pleural
thickening
However, CT can help distinguish between pleural
effusion and pleural empyema
45.
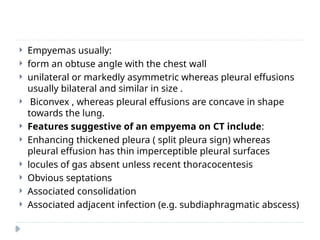
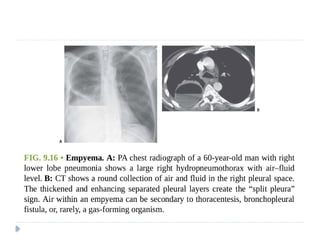
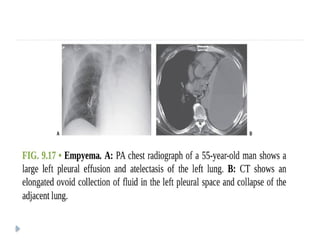
Empyemas usually:
form an obtuse angle with the chest wall
unilateral or markedly asymmetric whereas pleural effusions
usually bilateral and similar in size .
Biconvex , whereas pleural effusions are concave in shape
towards the lung.
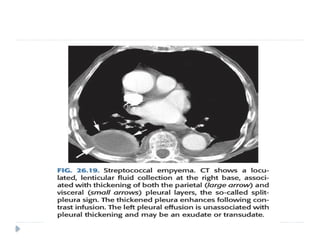
Features suggestive of an empyema on CT include:
Enhancing thickened pleura ( split pleura sign) whereas
pleural effusion has thin imperceptible pleural surfaces
locules of gas absent unless recent thoracocentesis
Obvious septations
Associated consolidation
Associated adjacent infection (e.g. subdiaphragmatic abscess)
Pneumothorax isdefined as a collection of air in the pleural
cavity
is divided into spontaneous and traumatic types
A pneumothorax occurring without an obvious precipitating
traumatic event or in a healthy individual is a primary
spontaneous pneumothorax.
This type of pneumothorax is strongly associated with smoking
and tall asthenic men
Most patients are between 20 and 40 years of age,
the male-to-female ratio is approximately 5:1
The cause is nearly always the rupture of an apical pleural bleb
Without treatment, the likelihood of another pneumothorax is
about 40%,
the chance of recurrence rises with each episode
61.
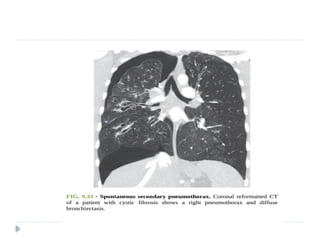
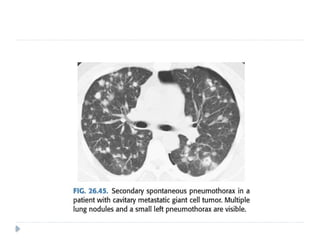
A pneumothoraxdeveloping without a
precipitating traumatic event in a patient with
predisposing lung disease is said to be a
spontaneous secondary pneumothorax .
Chronic obstructive pulmonary disease is the most
common cause of secondary spontaneous
pneumothorax.
pneumothoraces are associated with lung
metastases.( sarcomas most common) ,and some
cystic lung diseases.
62.
Catamenial pneumothoraxis an uncommon
disorder that occurs in women, probably caused
by air entering the peritoneal cavity by way of the
genital tract during menses and proceeding to
the pleural cavity through diaphragmatic
fenestrations.
Catamenial pneumothorax occurs only in relation
to the menses, appearing 1 day before or up to 3
days after menses.
The pneumothorax is usually small and most
often right-sided
63.
Tension pneumothorax:
Life threatening complication.
Diagnosis is usually made clinically
Tension pneumothorax is when there is a build-
up of positive pressure within the hemithorax,
to the extent that the lung is completely
collapsed, the diaphragm is flattened and the
mediastinum is distorted and, eventually, the
venous return to the heart is compromised.
Any pleural breach is inherently valve-like
because air will find its way out through the
alveoli but cannot be drawn back in because the
lung tissue collapses around the hole in the
64.
Iatrogenic causes
percutaneous biopsy
barotrauma (e.g. divers), ventilator
radiofrequency (RF) ablation of lung mass
endoscopic perforation of the oesophagus
central venous catheter insertion, nasogastric tube
placement
Traumatic causes
pulmonary laceration
Stab wound
Rib fracture
tracheobronchial rupture
oesophageal rupture
65.
Radiologic features
Aswith pleural effusion, the radiographic appearance of
pneumothorax depends on the radiographic projection, the
patient’s position, and the presence or absence of pleural
adhesion and subsequent loculation.
Plain radiograph
usually easily appreciated on erect chest radiographs.
Typically they demonstrate:
visible visceral pleural edge is seen as a very thin, sharp white
line
no lung markings are seen peripheral to this line
peripheral space is radiolucent compared to the adjacent lung
lung may completely collapse
mediastinum should not shift away from the pneumothorax
unless a tension pneumothorax is present
66.
CT
Providedlung windows are examined, a
pneumothorax is very easily identified on CT, and
should pose essentially no diagnostic difficulty.
pneumothorax is imaged as air in the pleural
space outside the lung and visceral pleura.
Even a very small pneumothorax is visible in the
anterior pleural space.
Its diagnosis is usually straightforward, although
differentiating a medial pneumothorax from
pneumomediastinun may be difficult in some
cases.
71.
Bronchopleural fistula
⚫Differs frompneumothorax in that the
communication with pleural space is via airways
rather than distal air spaces.
⚫Two main causes :
partial or complete lung resection
In association with necrotizing infections
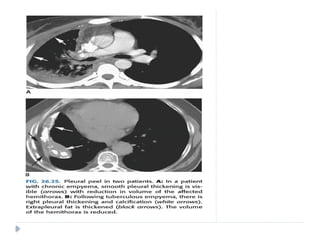
Pleural thickeningis common and is usually a sequel of
pleural inflammation.
It may also be a delayed complication of hemothorax,
pleural empyema, and recurrent pneumothorax.
Localized pleural thickening is frequently found at the
bases and results in blunting of the costophrenic angles
with tenting of the diaphragmatic pleura .
Fibrous pleural thickening is also common in the apical
pleural cupola where it may be secondary to
tuberculosis or represent age-related change.
These “apical pleural caps” sometimes have a scalloped
contour or may show slight tenting towards the lung
74.
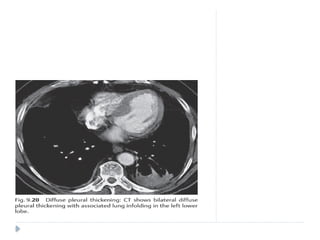
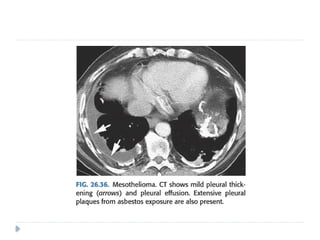
Asbestos relateddiffuse pleural thickening is much less
common than discrete pleural plaques and involves the
visceral rather than the parietal pleura
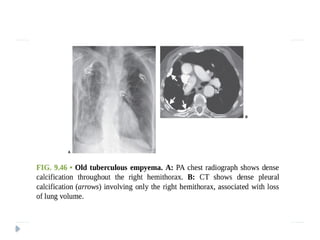
Evidence of underlying parenchymal disease is usually
seen in patients with prior tuberculosis or other
empyema.
Hemorrhagic effusion, tuberculosis, and other causes of
empyema usually lead to unilateral pleural abnormalities
benign asbestos pleurisy usually leads to bilateral pleural
Involvement of the mediastinal pleura is more common
with mesothelioma or other malignancies .
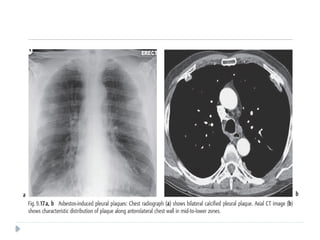
Pleural plaquesare circumscribed collections of dense
collagenous connective tissue, which may or may not be
calcified,
They represent the most common manifestation of and
serve as a biomarker of asbestos exposure
The latency period between exposure to asbestos and
development of pleural plaques is approximately 15 years.
The plaques involve mainly the posterior and
anterolateral aspects of the pleura, following the contours
of the posterolateral seventh to 10th ribs, and the domes
of the hemidiaphragms, and spare the lung apices and
costophrenic angles
81.
They almostalways involve only the parietal
pleura but occasionally may be seen in the
visceral pleura in the interlobar fissures and
sometimes involve the pericardium
On chest radiographs, pleural plaques are
unilateral in approximately 25% of cases
more plaques are detected on CT than chest
radiography.
82.
Pleural plaquesare not premalignant, but detection of
them is important for three main reasons:
(i) in patients with associated interstitial lung disease,
the presence of pleural plaques, in the proper clinical
and occupational setting, strongly suggests the
diagnosis of asbestosis;
(ii) they are virtually pathognomonic of asbestos
exposure and should prompt an occupational history
(iii) they may encourage a patient to stop smoking,
because there is a synergistic interaction between
asbestos exposure and smoking in the development
of lung cancer
83.
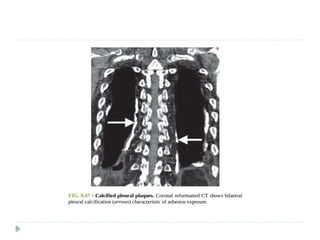
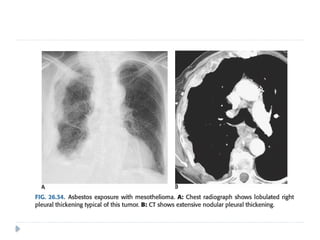
NB .Asbestos-related pleural disease has five
manifestations:
(i) pleural plaque with or without calcification,
(ii) asbestos-related pleural effusion,
(iii) diffuse pleural thickening,
(iv) rounded atelectasis,
(v) mesothelioma
84.
⚫PLEURAL PLAQUES CANBE CLASSIFI ED
ACCORDING TO THEIR CT APPEARANCE:
⚫Minimal pleural plaques: less than 1 mm thick, 1 to 3 cm
long, and few in number
⚫Moderate pleural plaques: 1 to 3 mm thick, 2 to 5 cm
long, and multiple
⚫Severe pleural plaques: thicker than 3 mm, clearly
indenting adjacent lung, up to 8 cm in craniocaudal
dimension, and extensive in width.
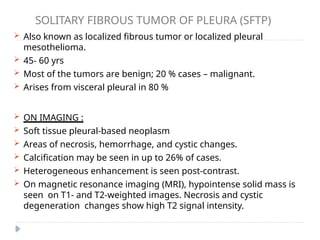
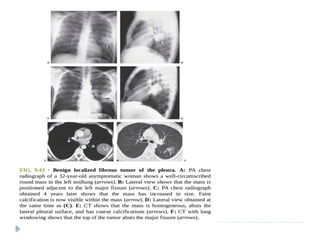
SOLITARY FIBROUS TUMOROF PLEURA (SFTP)
Also known as localized fibrous tumor or localized pleural
mesothelioma.
45- 60 yrs
Most of the tumors are benign; 20 % cases – malignant.
Arises from visceral pleural in 80 %
ON IMAGING :
Soft tissue pleural-based neoplasm
Areas of necrosis, hemorrhage, and cystic changes.
Calcification may be seen in up to 26% of cases.
Heterogeneous enhancement is seen post-contrast.
On magnetic resonance imaging (MRI), hypointense solid mass is
seen on T1- and T2-weighted images. Necrosis and cystic
degeneration changes show high T2 signal intensity.
96.
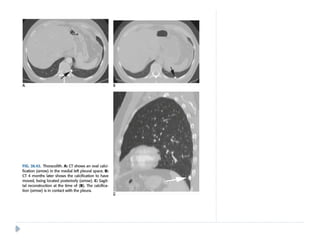
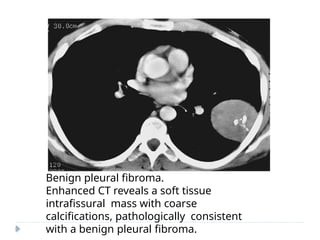
Benign pleural fibroma.
EnhancedCT reveals a soft tissue
intrafissural mass with coarse
calcifications, pathologically consistent
with a benign pleural fibroma.
97.
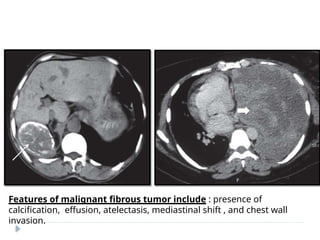
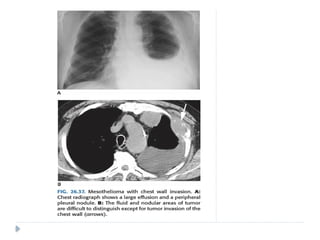
Features of malignantfibrous tumor include : presence of
calcification, effusion, atelectasis, mediastinal shift , and chest wall
invasion.
98.
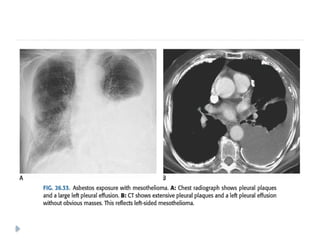
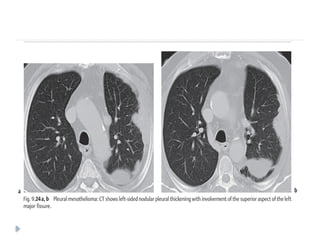
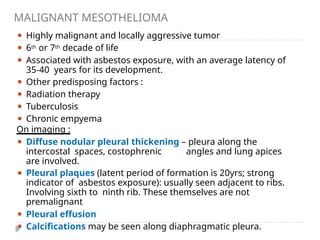
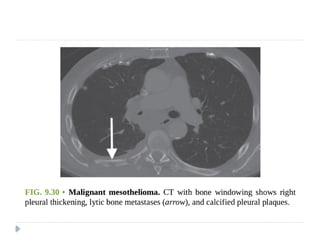
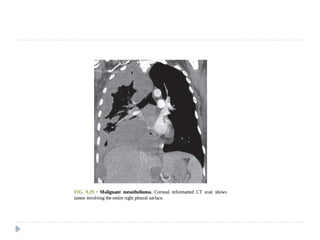
MALIGNANT MESOTHELIOMA
⚫ Highlymalignant and locally aggressive tumor
⚫ 6th or 7th decade of life
⚫ Associated with asbestos exposure, with an average latency of
35-40 years for its development.
⚫ Other predisposing factors :
⚫ Radiation therapy
⚫ Tuberculosis
⚫ Chronic empyema
On imaging :
⚫ Diffuse nodular pleural thickening – pleura along the
intercostal spaces, costophrenic angles and lung apices
are involved.
⚫ Pleural plaques (latent period of formation is 20yrs; strong
indicator of asbestos exposure): usually seen adjacent to ribs.
Involving sixth to ninth rib. These themselves are not
premalignant
⚫ Pleural effusion
⚫ Calcifications may be seen along diaphragmatic pleura.
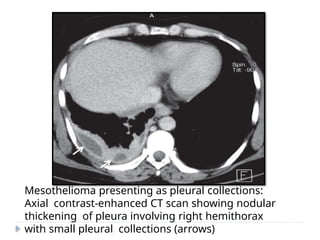
100.
Mesothelioma presenting aspleural collections:
Axial contrast-enhanced CT scan showing nodular
thickening of pleura involving right hemithorax
with small pleural collections (arrows)
104.
Malignant mesothelioma:
Axial contrast-enhancedCT scan showing enhancing
nodular pleural thickening (arrows) involving the
costal and mediastinal pleura, extending into the
major fissure (arrowhead) with crowding of ribs
108.
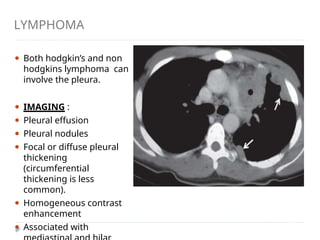
LYMPHOMA
⚫ Both hodgkin’sand non
hodgkins lymphoma can
involve the pleura.
⚫ IMAGING :
⚫ Pleural effusion
⚫ Pleural nodules
⚫ Focal or diffuse pleural
thickening
(circumferential
thickening is less
common).
⚫ Homogeneous contrast
enhancement
⚫ Associated with
109.
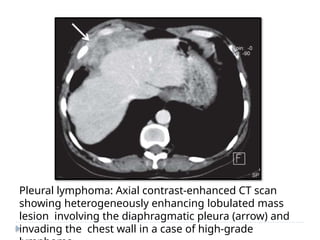
Pleural lymphoma: Axialcontrast-enhanced CT scan
showing heterogeneously enhancing lobulated mass
lesion involving the diaphragmatic pleura (arrow) and
invading the chest wall in a case of high-grade
110.
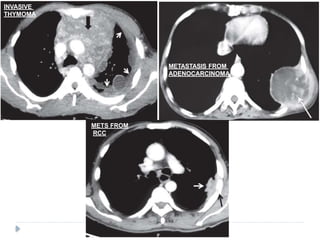
PLEURAL METASTASES
⚫ Adenocarcinomasare known to cause pleural
metastasis than any other histological types of
cancers.
⚫ Common primary sites are from : lung, lymphoma,
and ovary, invasive thymoma
⚫ Pleural effusion is the most common finding on
imaging .
ASKIN TUMOR
⚫ Aggressivemalignant tumor of primitive
neuroectodermal origin.
⚫ Mostly arise from the soft tissues of the chest wall or
lung
periphery.
⚫ Children & adolescents.
⚫ IMAGING :
⚫ U/L involvement usually seen
⚫ Nodular pleural thickening
⚫ Infiltration into the chest wall, mediastinum and
sympathetic chain is pathognomic.
⚫ Pleural effusion and rib destruction may or may
not be seen.
116.
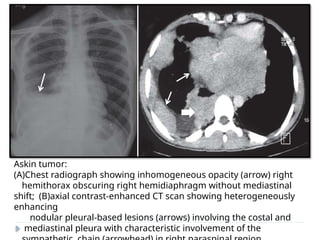
Askin tumor:
(A)Chest radiographshowing inhomogeneous opacity (arrow) right
hemithorax obscuring right hemidiaphragm without mediastinal
shift; (B)axial contrast-enhanced CT scan showing heterogeneously
enhancing
nodular pleural-based lesions (arrows) involving the costal and
mediastinal pleura with characteristic involvement of the
117.
RARE PATHOLOGIES OFPLEURA
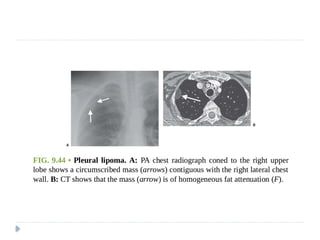
1) PLEURAL LIPOMA (often an incidental finding; one of the
most common benign tumors of the pleura; fat density
tissue with no contrast enhancement)
2) PLEURAL SPLENOSIS (occurs following trauma on left side)
3) MESOTHELIAL CYSTS
4) EPITHELIOID HEMANGIOENDOTHELIOMA
5) CASTLEMAN DISEASE
6) SARCOMAS
7) MALIGNANTG FIBROUS HISTIOCYTOMA
8) LEUKEMIC INFILTRATION
9) EXTRASKELETAL OSTEOSARCOMA (RARE: but should be
considered in the differential diagnosis for a rapidly growing
calcified pleural mass in an elderly)
120.
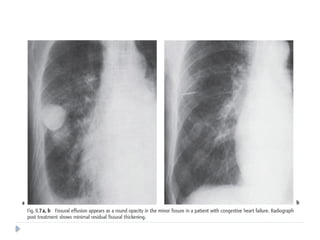
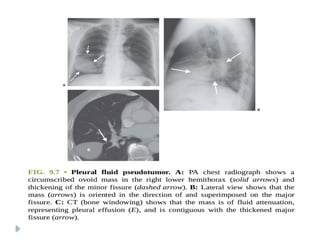
PLEURAL PSEUDOTUMOR
⚫ Isa fluid collection within the lung fissure.
⚫ Most common site : MINOR FISSURE
⚫ Common causes include :
Congestive heart failure
Cirrhosis
Renal insufficiency
⚫ On chest radiographs:
⚫ Classical lenticular or biconvex opacity is seen in
the fissure.
⚫ Usually resolves after therapy with diuretic
agents



























































![carotid stenosis [Autosaved].pptx for master students](https://cdn.slidesharecdn.com/ss_thumbnails/carotidstenosisautosaved-241229032708-f20dd02c-thumbnail.jpg?width=640&height=640&fit=bounds)




















