Downloaded 47 times














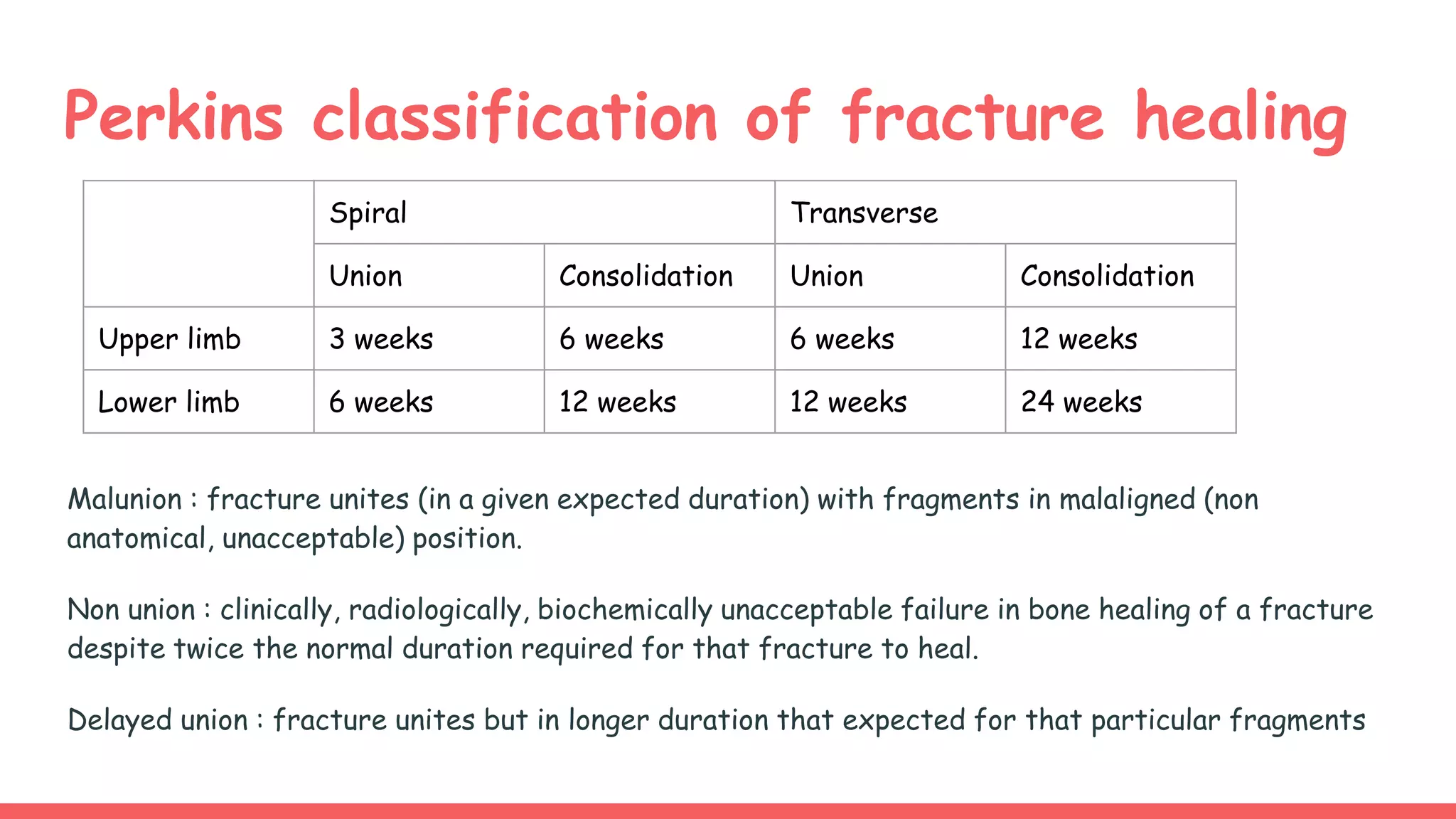



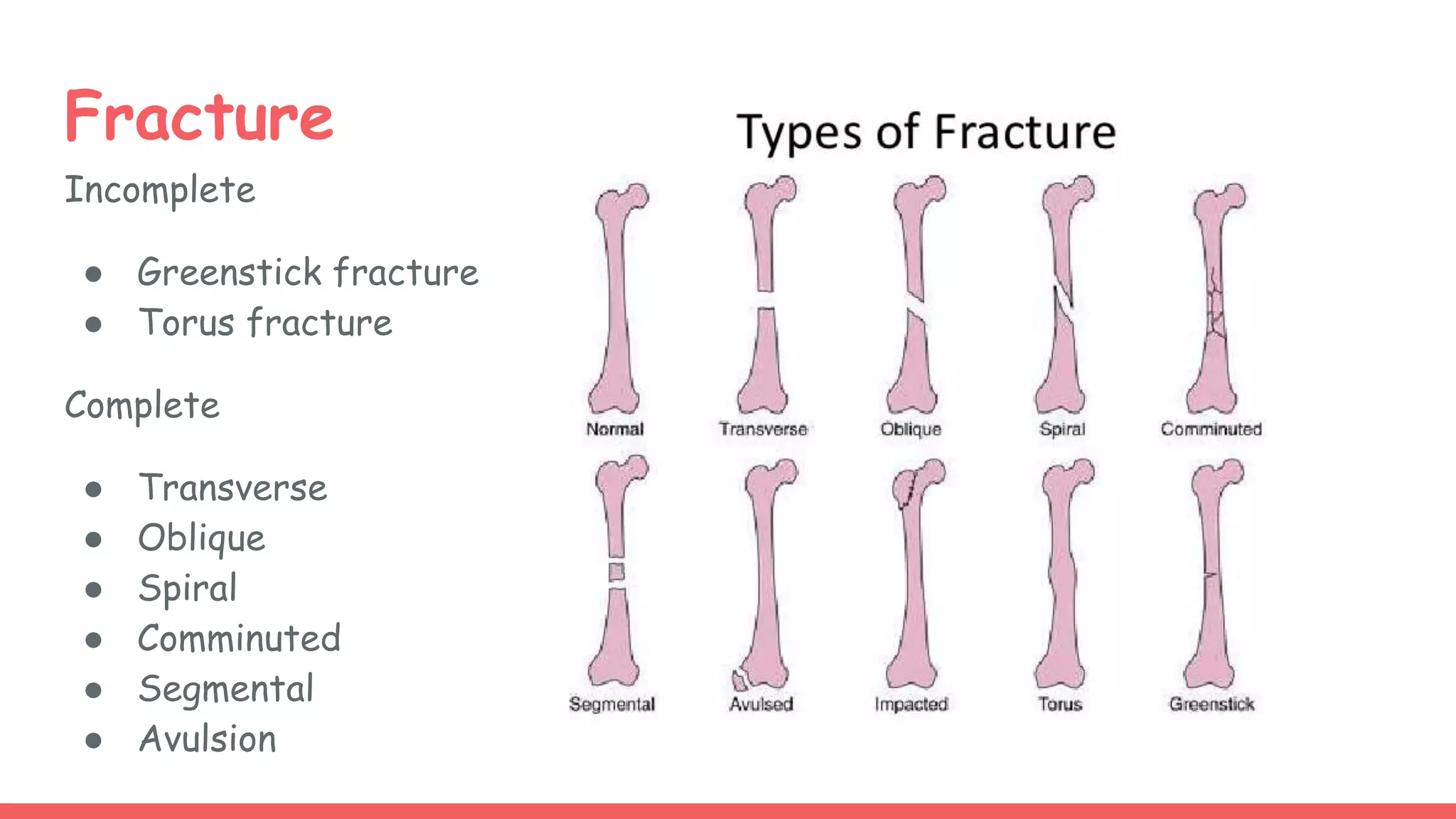




















Bone is composed of organic and inorganic components and water. It undergoes constant metabolism regulated by hormones like parathyroid hormone and calcitonin. Fractures are breaks in bone continuity and are classified based on features like displacement and soft tissue involvement. Treatment involves reduction, immobilization with splints or internal fixation, and rehabilitation. Complications can include delayed healing, malunion, and secondary osteoarthritis if not managed properly.











































































