Downloaded 386 times






1. Bleeding in early pregnancy can be caused by miscarriage, ectopic pregnancy, or rare conditions like cervical cancer or polyps. 2. Miscarriage is the most common cause, and it is defined as the natural or spontaneous end of a pregnancy before 24 weeks. Early pregnancy assessment using transvaginal ultrasound and serum hCG levels can help diagnose the cause. 3. Ectopic pregnancies, which occur when a fertilized egg implants outside the uterus, should also be considered and ruled out as they can be life-threatening if ruptured. Transvaginal ultrasound and serial hCG measurements are used to diagnose ectopic pregnancies.






































































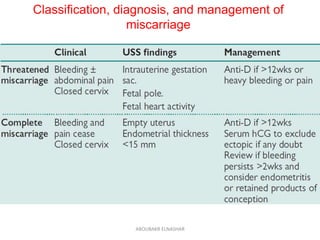
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















