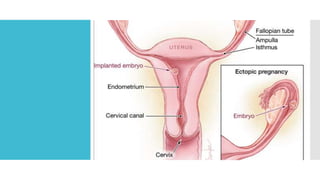
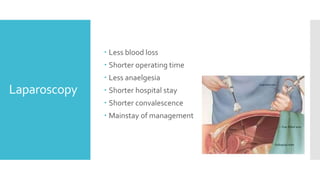
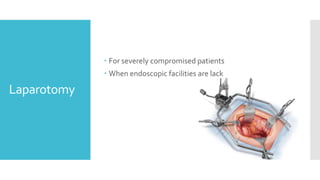
An ectopic pregnancy occurs when a conceptus implants outside the uterine cavity, primarily in the fallopian tubes. Risk factors include tubal disease, previous ectopic pregnancies, and use of intrauterine devices, presenting clinically with abdominal pain and vaginal bleeding. Management options are based on the patient's condition and include expectant, medical, or surgical approaches depending on factors like hCG levels and ultrasound findings.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








