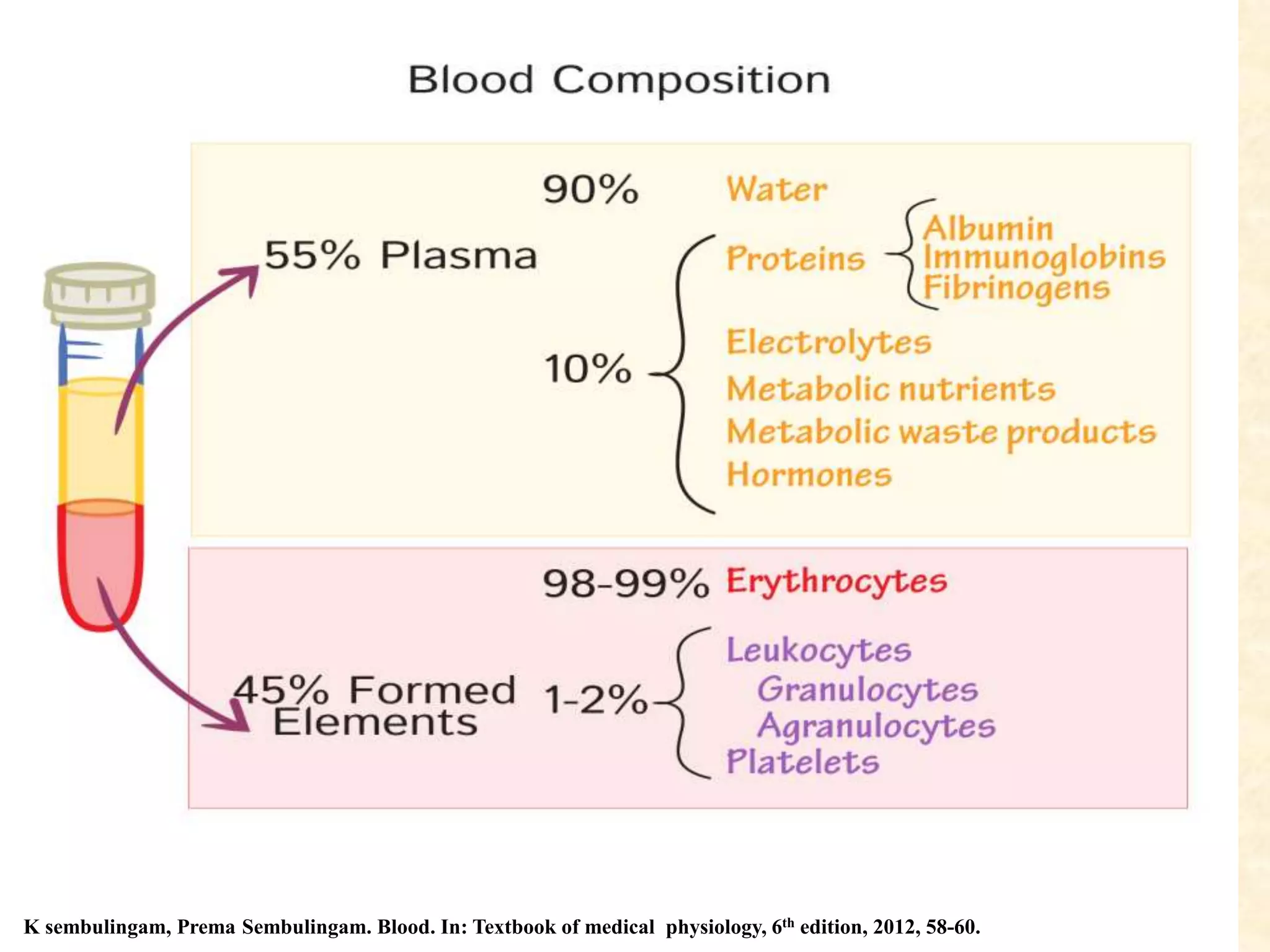
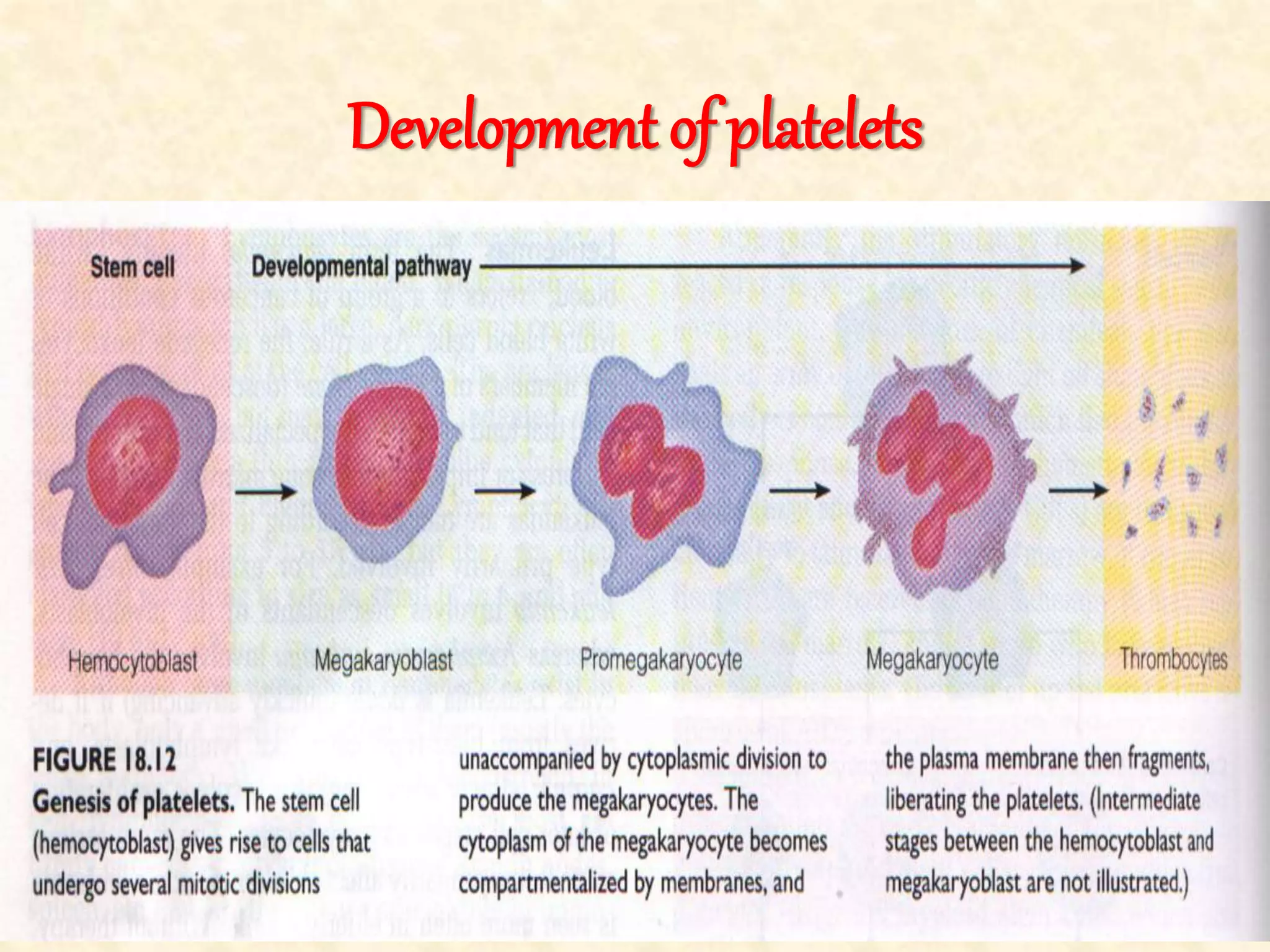
The document discusses bleeding and coagulation. It defines blood and its components like plasma, red blood cells, white blood cells and platelets. It describes the processes of erythropoiesis, the formation of red blood cells in the bone marrow, and hemostasis, the prevention of blood loss through vascular constriction, platelet plug formation and blood clotting. It also discusses the clotting factors involved in the coagulation cascade and the mechanisms of platelet activation, shape change, secretion and aggregation that form the platelet plug during hemostasis.