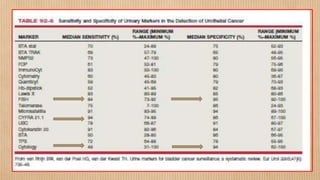
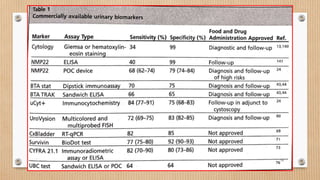
Urinary biomarkers are being developed and used as noninvasive alternatives to cystoscopy for bladder cancer diagnosis and monitoring. While no single biomarker has shown better specificity than urine cytology, many have higher sensitivity. Commonly used biomarkers include NMP22, BTA stat, ImmunoCyt/uCyt+, and UroVysion, with UroVysion and telomerase showing promise in sensitivity and specificity. An ideal biomarker would be noninvasive, highly sensitive and specific, easy to perform, rapid, reproducible, cost-effective, and able to detect cancer before it becomes visible on cystoscopy. Currently, biomarkers are used alongside cystoscopy for surveillance of non-muscle invasive bladder cancer, and may anticipate








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















