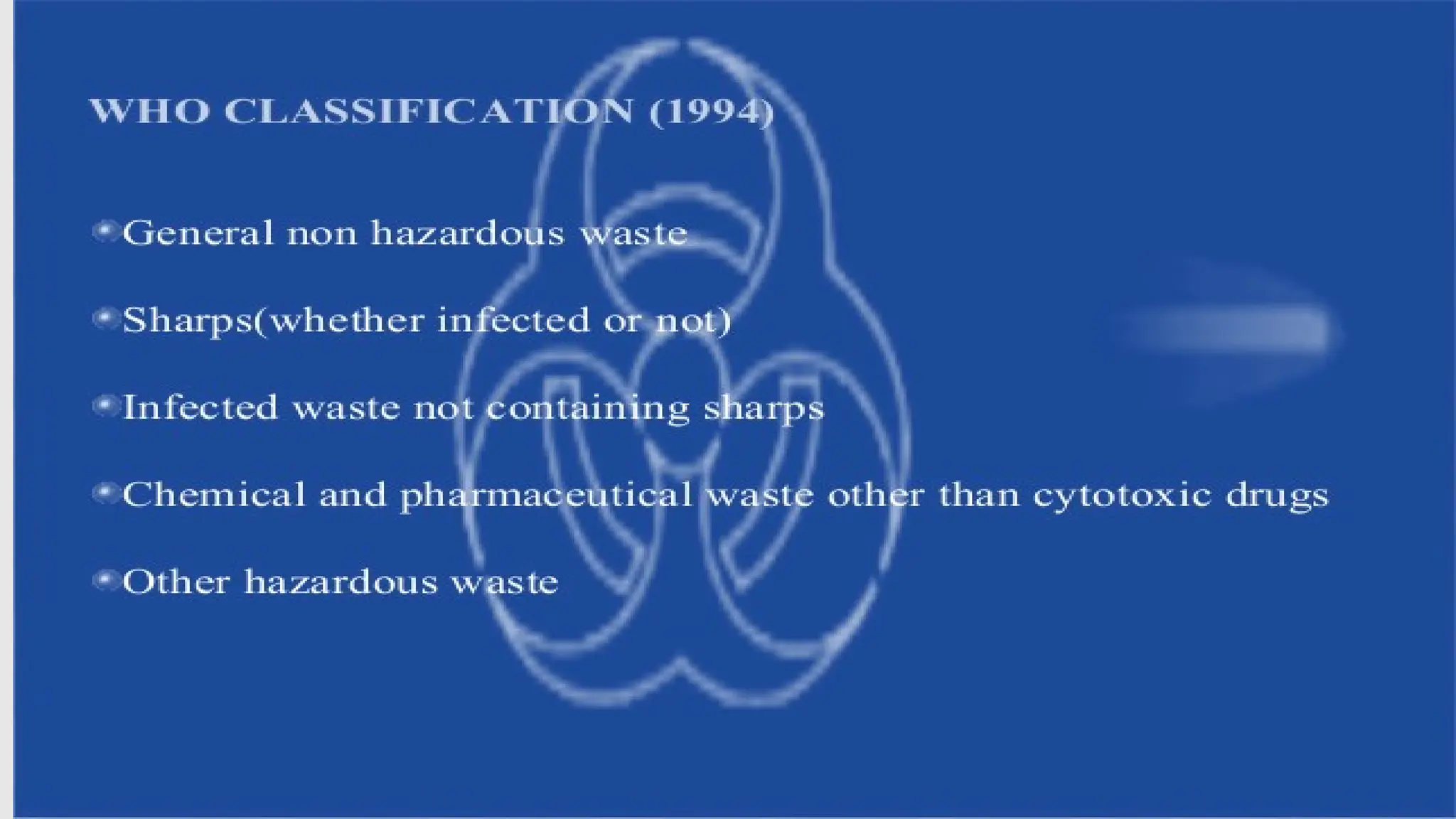
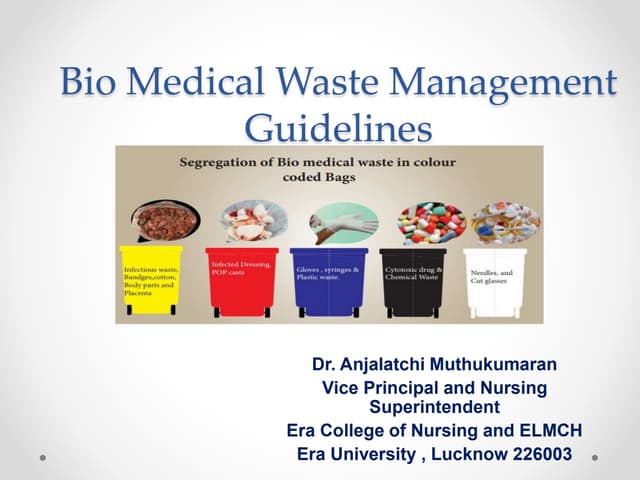
The document provides an overview of biomedical waste (BMW) management, its classification, and the associated risks in India. It highlights the legislative framework, the impact of COVID-19 on BMW handling, and emphasizes the importance of proper waste segregation to mitigate environmental threats. Key guidelines for the treatment, storage, and disposal of biomedical waste during the pandemic are also discussed.