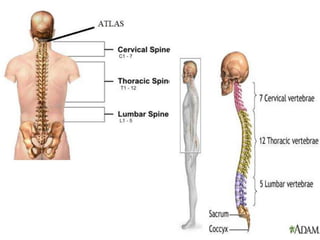
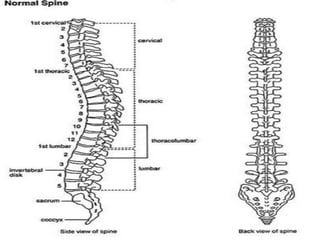
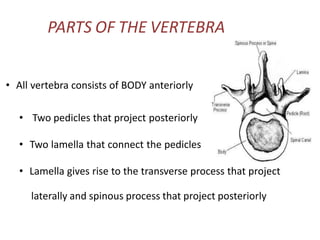
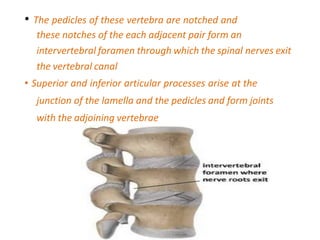
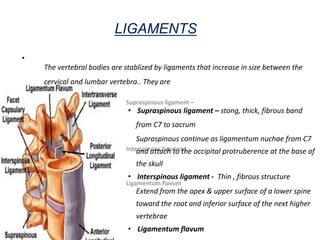
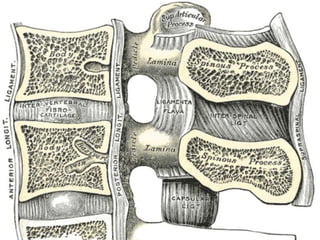
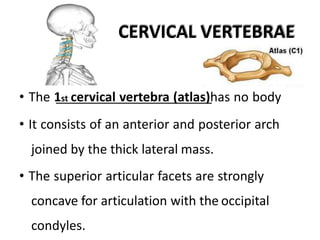
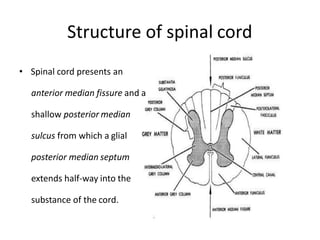
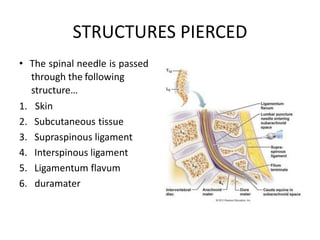
The document provides information on the anatomy and physiology of the spinal cord and vertebral column. It discusses the parts of the vertebrae including the body, pedicles, lamina, processes and joints. It describes the ligaments that support the spine like the supraspinous, interspinous and ligamentum flavum. It details the characteristics of cervical, thoracic, lumbar and sacral vertebrae. It also discusses the meninges layers, cerebrospinal fluid, vertebral anomalies and embryology of spinal development.


















































![[3] The Back and ANS.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/3thebackandans-230325182407-aaf75a6c-thumbnail.jpg?width=640&height=640&fit=bounds)



















