

The document outlines the key elements that should be included in a bioequivalence study protocol. It discusses the study objective to show that the drug bioavailability from test and reference products is statistically equivalent. The study design may include crossover, parallel, or replicate designs. Important aspects covered include the study population, drug administration, sampling schedule, analytical methods, data analysis plan, and statistical evaluation of pharmacokinetic parameters to determine bioequivalence within the 80-125% range. In vitro dissolution and content uniformity testing should also be included to support the in vivo bioequivalence results.
Introduction to the bioequivalence protocol presented by T.M. Rasala, focusing on its significance.
Elements including study title, objectives, design, population, procedures, ethical considerations, data analysis, and facilities.
The aim is to show no statistical difference in drug bioavailability between test and reference products given under similar conditions.
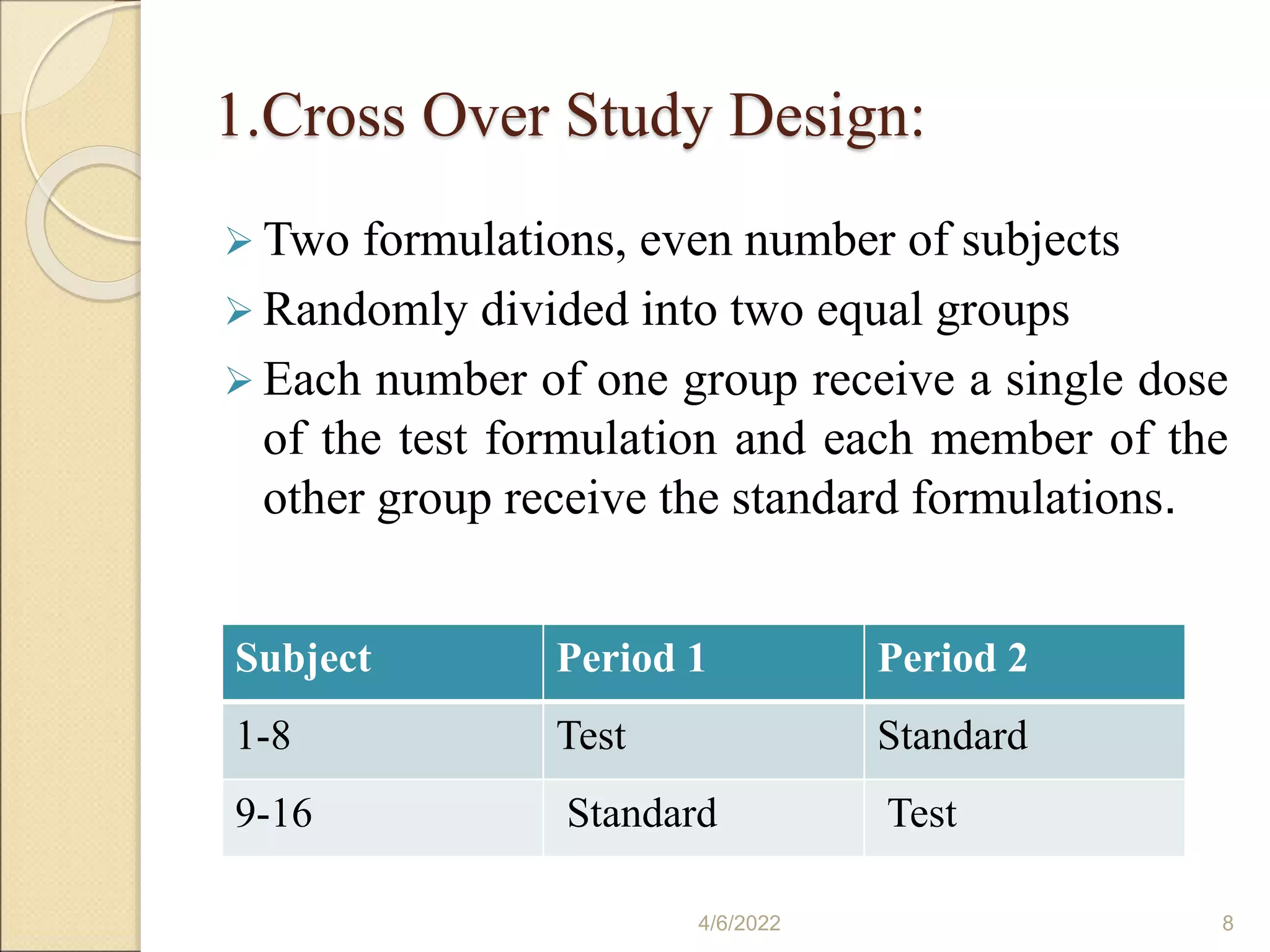
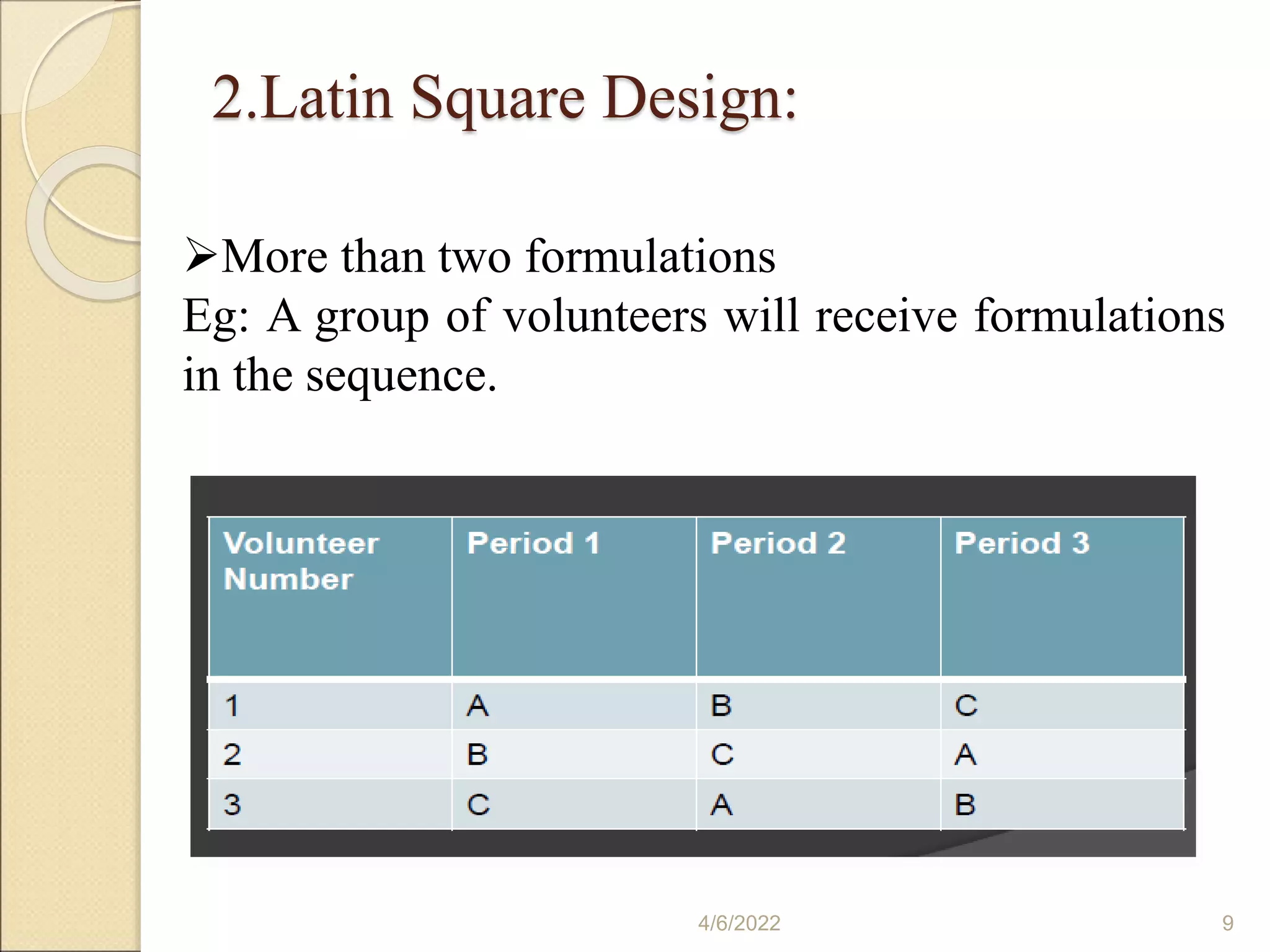
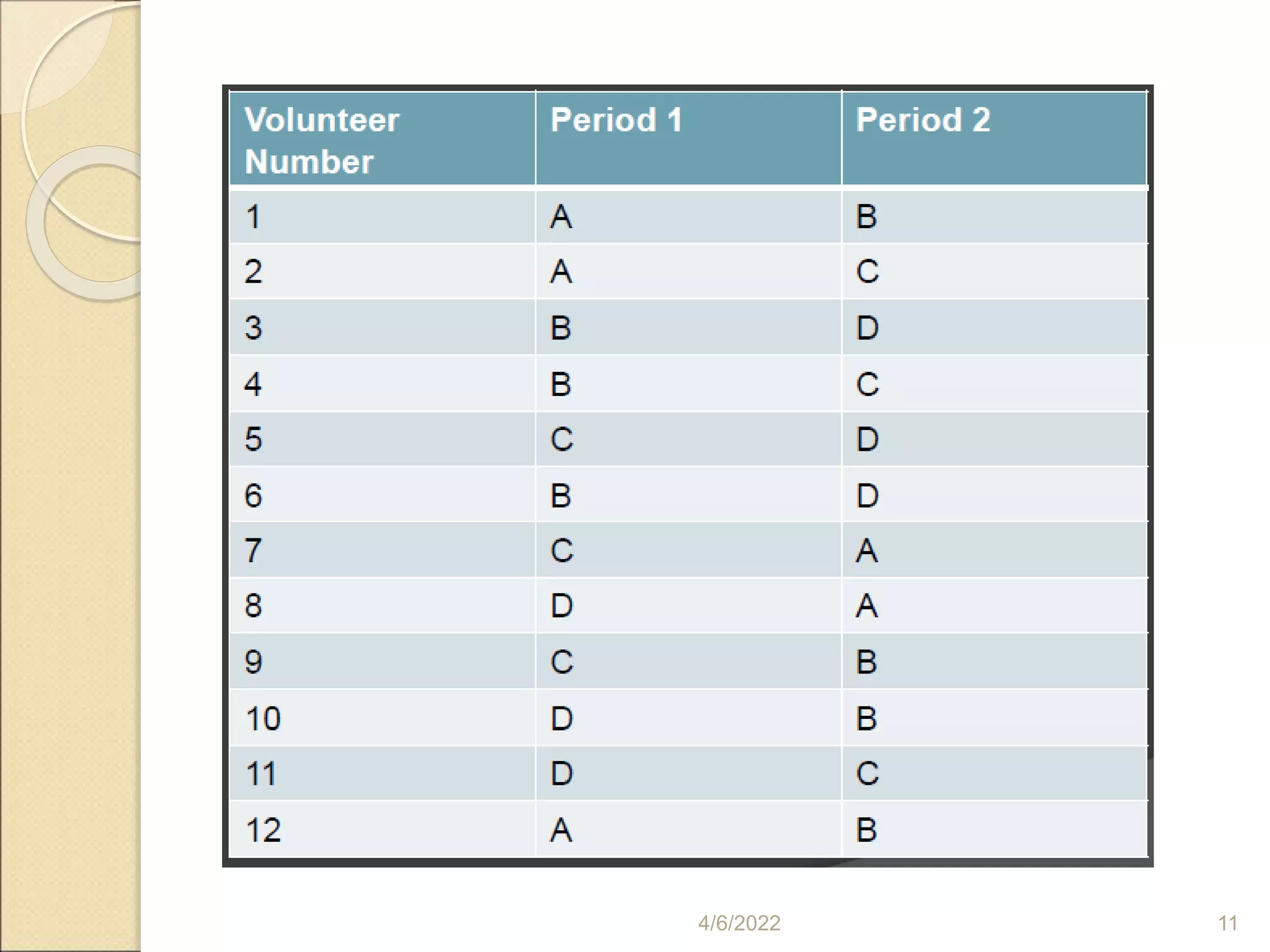
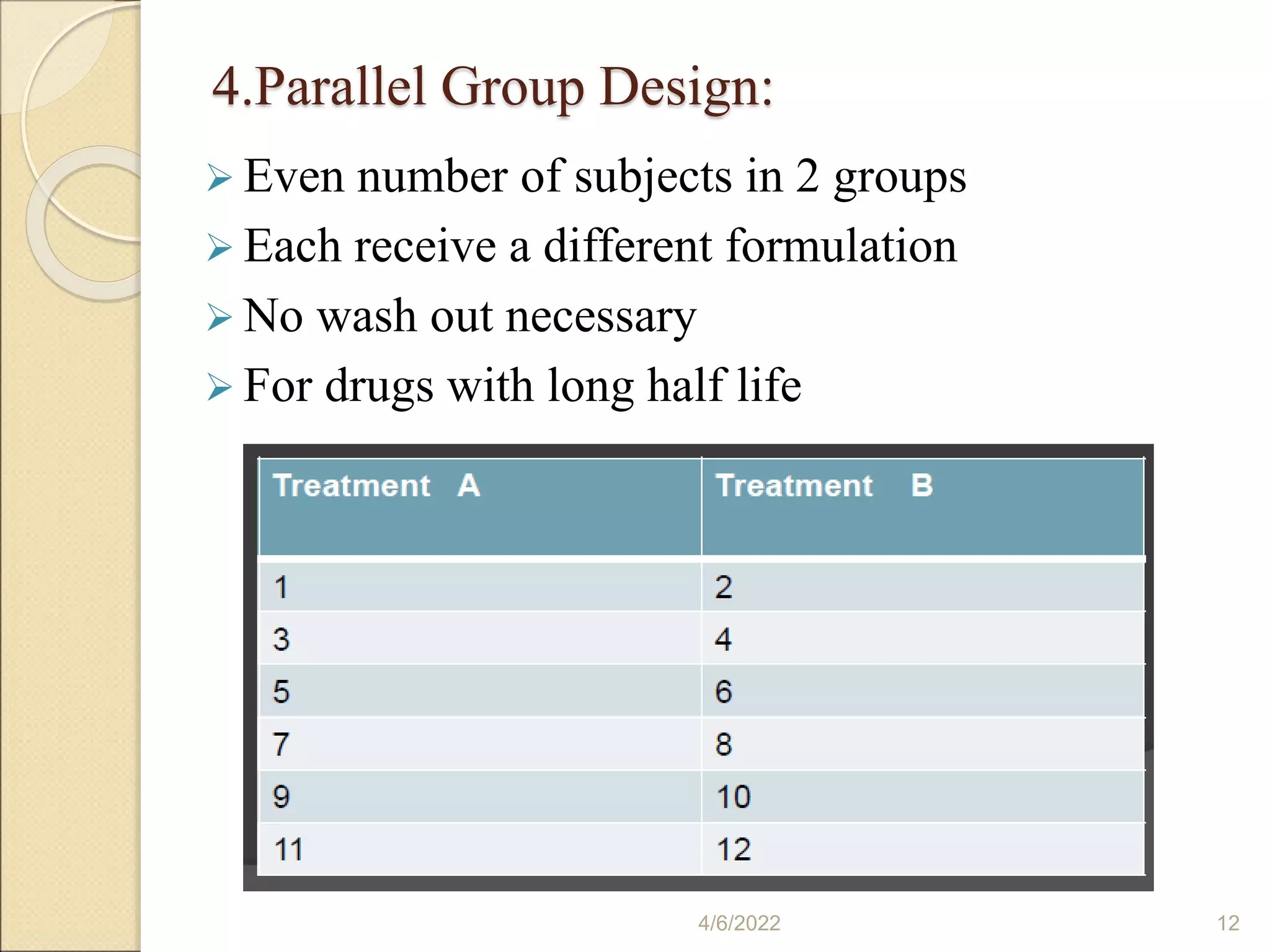
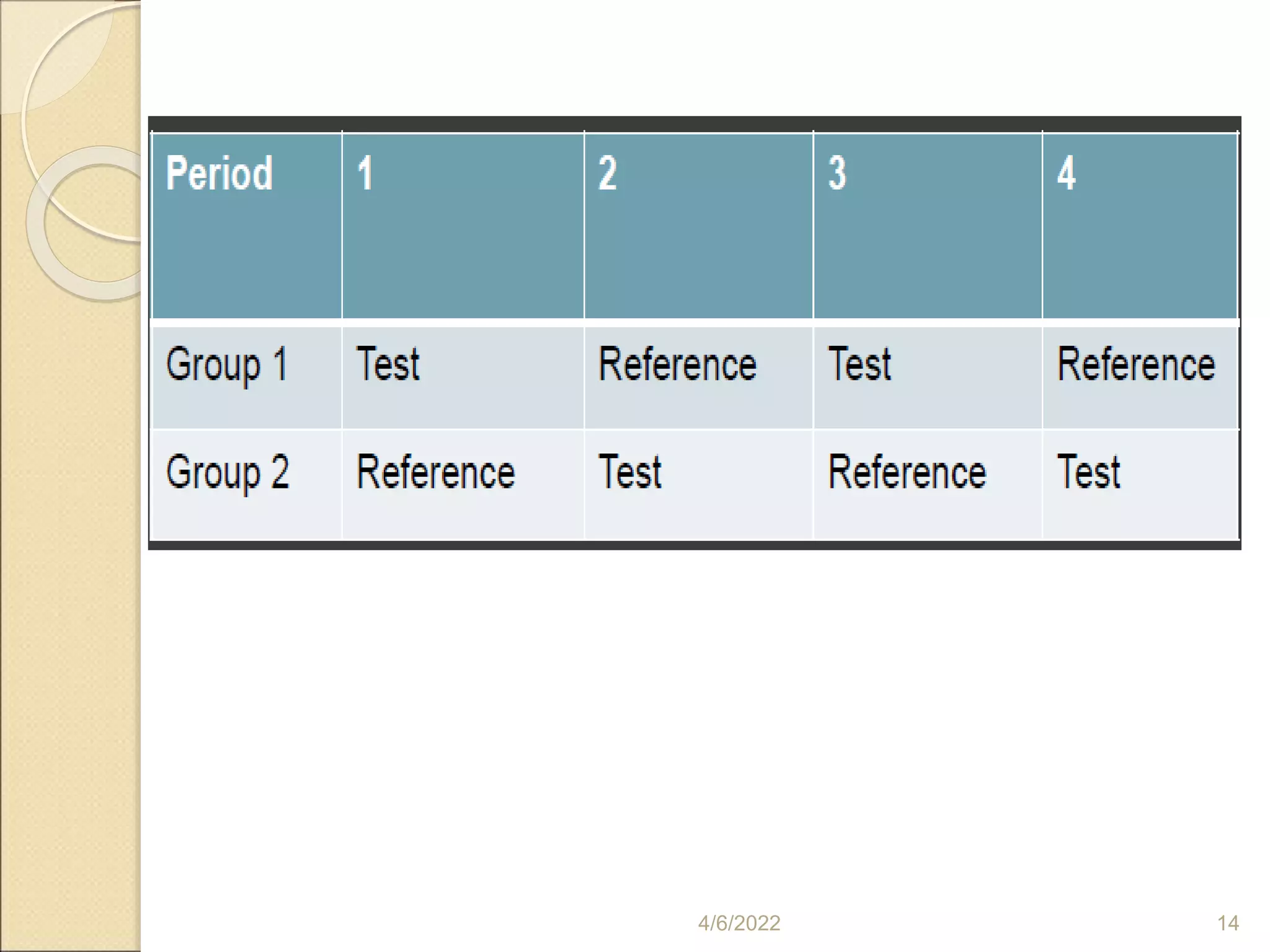
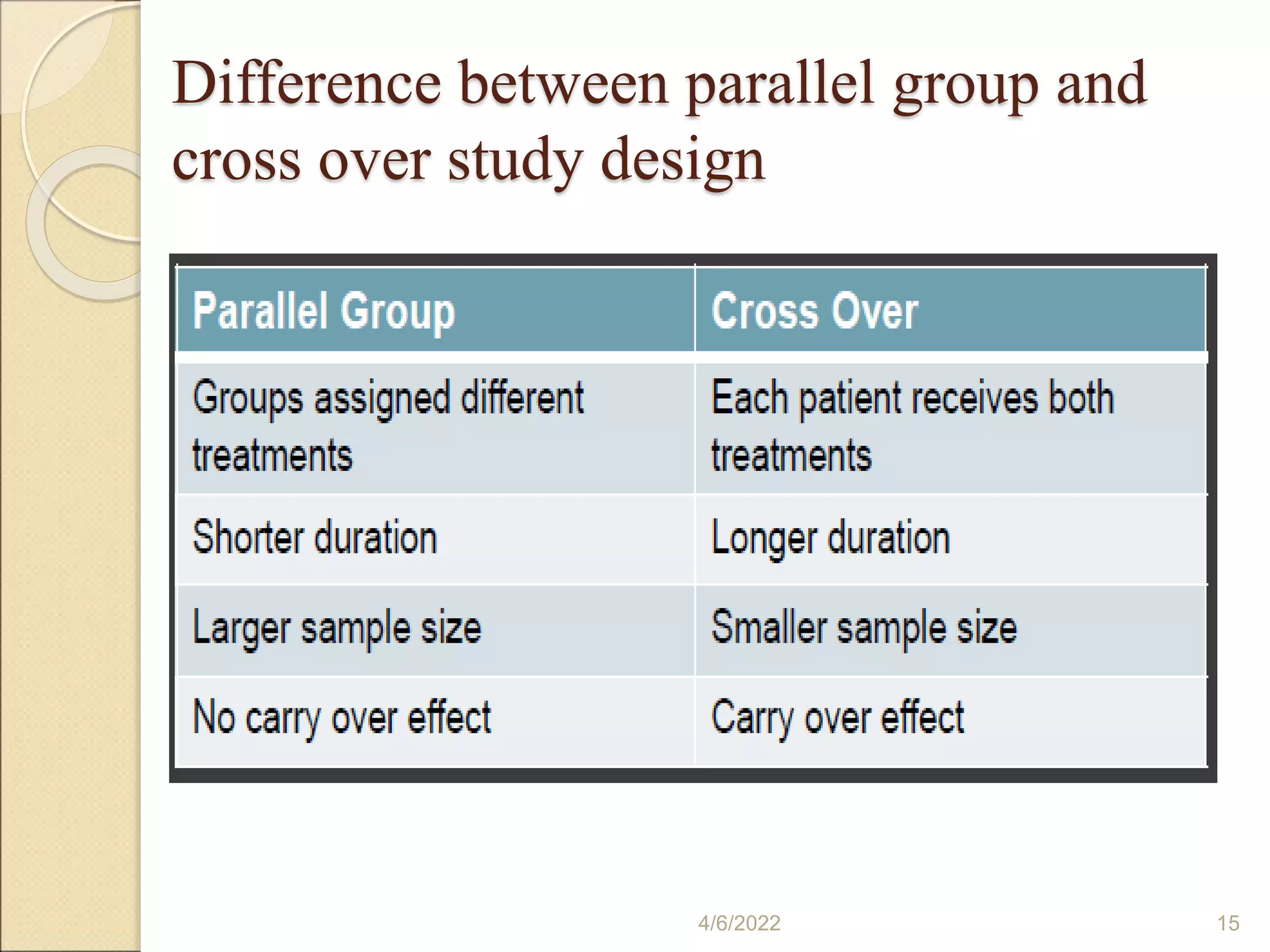
Variety of study designs, including fasting, food intervention, and multi-dose studies, with details of crossover, square, and group designs.
Guidelines for subject selection in studies, addressing age, health status, and inclusion/exclusion criteria.
Randomization and administration of drug products, emphasizing the impact of timing on drug concentration measurements.
Determination of biological samples for drug absorption evaluation, addressing sampling methods and limitations.
Pharmacokinetic analyses involved in studying single-dose bioequivalence, focusing on AUC and Cmax metrics.
Required components for in-vivo bioequivalence study submissions, including protocols, approvals, and statistical analysis.
Details on pharmacokinetic parameters, statistical assessments, analyses of variance, and recommendations for reporting outcomes.



































































