Bioavailability is defined as the rate and extent to which an active drug reaches systemic circulation. Objectives of bioavailability studies include developing new formulations and determining the effects of excipients, patient factors, and drug interactions on absorption. Bioavailability can be assessed using pharmacokinetic methods like determining blood concentrations over time to calculate AUC, Cmax, and Tmax, or by measuring urinary drug excretion. Bioequivalence studies establish equivalence between test and reference drug products using randomized crossover or parallel designs in accordance with regulatory guidelines. Key parameters compared include AUC, Cmax, and the time to reach Cmax to ensure bioequivalent drug products have similar rates and extents of absorption.
FORMULATION FACTORS EFFECTING BIOAVAILABILITY OF DRUGSN Anusha
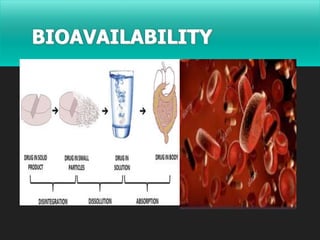
Bioavailability means the rate and extent to which the active ingredient is absorbed from a drug product and becomes available at the site of action.
When the drug is given orally, only part of the administered dose appears in the plasma.
By plotting plasma concentrations of the drug versus time, one can measure the area under the curve (AUC).
This curve reflects the extent of absorption of the drug.
1. Measurement of Bioavailability:
Direct and indirect methods may be used to assess drug bioavailability. The in-vivo bioavailability of a drug product is demonstrated by the rate and extent of drug absorption, as determined by comparison of measured parameters, e.g., concentration of the active drug ingredient in the blood, cumulative urinary excretion rates, or pharmacological effects.
For drug products that are not intended to be absorbed into the bloodstream, bioavailability may be assessed by measurements intended to reflect the rate and extent to which the active ingredient or active moiety becomes available at the site of action.
The design of the bioavailability study depends on the objectives of the study, the ability to analyze the drug (and metabolites) in biological fluids, the pharmacodynamics of the drug substance, the route of drug administration, and the nature of the drug product.
Pharmacokinetic and/or pharmacodynamic parameters as well as clinical observations and in-vitro studies may be used to determine drug bioavailability from a drug product.
1.1. Pharmacokinetic methods:
These are very widely used and based upon the assumption that the pharmacokinetic profile reflects the therapeutic effectiveness of a drug. Thus these are indirect methods. The two major pharmacokinetic methods are:
The major pharmacokinetic methods are:
Plasma / blood level time profile.
o Time for peak plasma (blood) concentration (t max)
o Peak plasma drug concentration (Cmax)
o Area under the plasma drug concentration–time curve (AUC)
Urinary excretion studies.
o Cumulative amount of drug excreted in the urine (Du)
o Rate of drug excretion in the urine (dDu/dt)
o Time for maximum urinary excretion (t)
C. Other biological fluids
1.2. Pharmacodynamic methods:
IT involves direct measurement of drug effect on a (patho) physiological process as a function of time. Disadvantages of it may be high variability, difficult to measure, limited choices, less reliable, more subjective, drug response influenced by several physiological & environmental factors.
They involve determination of bioavailability from:
Acute pharmacological response.
Therapeutic response.
1.3. In-vitro dissolution studies
Closed compartment apparatus
Open compartment apparatus
Dialysis systems.
1.4. Clinical observations
Well-controlled clinical trials
Pharmacokinetics variations in Disease States.Faizan Akram
The biggest issue in PK/PD and drug therapy is variability in
response. Variability factors that affect pharmacokinetics and pharmacodynamics influence clinical trials and dose regimen designs.
FORMULATION FACTORS EFFECTING BIOAVAILABILITY OF DRUGSN Anusha
Bioavailability means the rate and extent to which the active ingredient is absorbed from a drug product and becomes available at the site of action.
When the drug is given orally, only part of the administered dose appears in the plasma.
By plotting plasma concentrations of the drug versus time, one can measure the area under the curve (AUC).
This curve reflects the extent of absorption of the drug.
1. Measurement of Bioavailability:
Direct and indirect methods may be used to assess drug bioavailability. The in-vivo bioavailability of a drug product is demonstrated by the rate and extent of drug absorption, as determined by comparison of measured parameters, e.g., concentration of the active drug ingredient in the blood, cumulative urinary excretion rates, or pharmacological effects.
For drug products that are not intended to be absorbed into the bloodstream, bioavailability may be assessed by measurements intended to reflect the rate and extent to which the active ingredient or active moiety becomes available at the site of action.
The design of the bioavailability study depends on the objectives of the study, the ability to analyze the drug (and metabolites) in biological fluids, the pharmacodynamics of the drug substance, the route of drug administration, and the nature of the drug product.
Pharmacokinetic and/or pharmacodynamic parameters as well as clinical observations and in-vitro studies may be used to determine drug bioavailability from a drug product.
1.1. Pharmacokinetic methods:
These are very widely used and based upon the assumption that the pharmacokinetic profile reflects the therapeutic effectiveness of a drug. Thus these are indirect methods. The two major pharmacokinetic methods are:
The major pharmacokinetic methods are:
Plasma / blood level time profile.
o Time for peak plasma (blood) concentration (t max)
o Peak plasma drug concentration (Cmax)
o Area under the plasma drug concentration–time curve (AUC)
Urinary excretion studies.
o Cumulative amount of drug excreted in the urine (Du)
o Rate of drug excretion in the urine (dDu/dt)
o Time for maximum urinary excretion (t)
C. Other biological fluids
1.2. Pharmacodynamic methods:
IT involves direct measurement of drug effect on a (patho) physiological process as a function of time. Disadvantages of it may be high variability, difficult to measure, limited choices, less reliable, more subjective, drug response influenced by several physiological & environmental factors.
They involve determination of bioavailability from:
Acute pharmacological response.
Therapeutic response.
1.3. In-vitro dissolution studies
Closed compartment apparatus
Open compartment apparatus
Dialysis systems.
1.4. Clinical observations
Well-controlled clinical trials
Pharmacokinetics variations in Disease States.Faizan Akram
The biggest issue in PK/PD and drug therapy is variability in
response. Variability factors that affect pharmacokinetics and pharmacodynamics influence clinical trials and dose regimen designs.
Methods For Assesment Of Bioavailability Anindya Jana
Bioavailability means the rate and extent to which the active ingredient or active moiety is absorbed from a drug product and becomes available at the site of action. For drug products that are not intended to be absorbed into the bloodstream, bioavailability may be assessed by measurements intended to reflect the rate and extent to which the active ingredient or active moiety becomes available at the site of action.
Bioavailability studies are important in the Primary stages of development of a suitable dosage form for a new drug entity, determination of influence of excipients, patient related factors & possible interaction with other drugs on the efficiency of absorption, development of new formulations of the existing drugs, control of quality of a drug product during the early stages of marketing in order to determine the influence of processing factors, storage & stability on drug absorption
CHRONOPHARMACOKINETICS AND TIME DEPENDENT PHARMACOKINETICSN Anusha
Chronopharmacokinetic studies have been demonstrating that time of administration is a possible factor of variation in the kinetics of the drug.
It entails the study of temporal changes in drug absorption, distribution, metabolism and elimination.
It investigates the variation in drug plasma levels as a function of time of day and the mechanisms responsible for time dependant variations.
The term circadian coined by Franz Halberg, comes from Latin.
“Circa” means around &“diem” means day.
An in-vitro in-vivo correlation (IVIVC) has been defined by the U.S. Food and Drug Administration (FDA) as "a predictive mathematical model describing the relationship between an in-vitro property of a dosage form and an in-vivo response".
"Application of pharmacokinetics and bioavailability in clinical situations"Faizan Akram
The success of drug therapy is highly dependent on the choice of the drug, the drug product, and the design of the dosage regimen. The choice of the drug is generally made by the physician after careful patient diagnosis and physical assessment. The choice of the drug product (eg, immediate release vs modified release) and dosage regimen is based on the patient’s individual characteristics and known pharmacokinetics.
Methods For Assesment Of Bioavailability Anindya Jana
Bioavailability means the rate and extent to which the active ingredient or active moiety is absorbed from a drug product and becomes available at the site of action. For drug products that are not intended to be absorbed into the bloodstream, bioavailability may be assessed by measurements intended to reflect the rate and extent to which the active ingredient or active moiety becomes available at the site of action.
Bioavailability studies are important in the Primary stages of development of a suitable dosage form for a new drug entity, determination of influence of excipients, patient related factors & possible interaction with other drugs on the efficiency of absorption, development of new formulations of the existing drugs, control of quality of a drug product during the early stages of marketing in order to determine the influence of processing factors, storage & stability on drug absorption
CHRONOPHARMACOKINETICS AND TIME DEPENDENT PHARMACOKINETICSN Anusha
Chronopharmacokinetic studies have been demonstrating that time of administration is a possible factor of variation in the kinetics of the drug.
It entails the study of temporal changes in drug absorption, distribution, metabolism and elimination.
It investigates the variation in drug plasma levels as a function of time of day and the mechanisms responsible for time dependant variations.
The term circadian coined by Franz Halberg, comes from Latin.
“Circa” means around &“diem” means day.
An in-vitro in-vivo correlation (IVIVC) has been defined by the U.S. Food and Drug Administration (FDA) as "a predictive mathematical model describing the relationship between an in-vitro property of a dosage form and an in-vivo response".
"Application of pharmacokinetics and bioavailability in clinical situations"Faizan Akram
The success of drug therapy is highly dependent on the choice of the drug, the drug product, and the design of the dosage regimen. The choice of the drug is generally made by the physician after careful patient diagnosis and physical assessment. The choice of the drug product (eg, immediate release vs modified release) and dosage regimen is based on the patient’s individual characteristics and known pharmacokinetics.
Bioavailability & Bioequivalence Studies
https://youtube.com/vishalshelke99
https://instagram.com/vishal_stagram
Sub :- Research Methodology
M.Phrmacy Semister 1
Savitribai Phule Pune University
Bioavailability:
Bioavailability is defined as a measure, of the rate and amount of drug, which reaches the systemic circulation unchanged following the administration of a dosage form.
Absolute bioavailability:
When systemic availability of a drug administered orally
is determined in comparison to its I.V. administration, denoted by F.
Relative bioavailability:
When systemic availability of a drug after oral administration is
Compared with that of oral standard of the same drug
( Solution or suspension ) and denoted by Fr.
Measurement of bioavailability and concept of equivalenceRavish Yadav
The all the content in this profile is completed by the teachers, students as well as other health care peoples.
thank you, all the respected peoples, for giving the information to complete this presentation.
this information is free to use by anyone.
Bioavailability & Bioequivalence ppt, Objectives, Improving bioavailability, Assessment of bioavailability, Urinary excretion studies, Blood serum studies, in vitro drug dissolution testing, need for dissolution testing, in vitro drug dissolution testing models, Bioequivalence, Therapeutic equivalence, Types of bioequivalence studies, Pharmacokinetic studies, Methods to enhance dissolution rate.
2. ❖ DEFINITION
● Bioavailability is defined as the rate and the
absorption of drug that reaches the biological
system in an active form, capable of exerting the
desired pharmacological effect, including its
onset, intensity and duration of its action.
3. Objectives of bioavailability studies:
• Development of new formulation.
• Determination of influence of excipients, patient
related factors and possible interaction with other
drugs on the efficiency of absorption.
• Control of quality of a drug product during the early
stages of marketing in order to determine the
influence of processing factors, storage, stability on
drug absorption.
• Primary stages of the development of a suitable
dosage form for a new drug entity.
4. • CONSIDERATIONS IN IN-VIVO BIOAVAILABILITY
STUDY DESIGN:
➢Bioavailability—Absolute versus Relative
• ABSOLUTE BIOAVAILABILITY:
• The systemic availability of a drug administered orally is determined in
comparison to its iv administration.
• Characterization of a drug's absorption properties from the e.v. site.
• F = AUCev
AUCiv
• RELATIVE BIOAVAILABILITY:
• The availability of a drug product as compared to another dosage form or
product of the same drug given in the same dose.
• Characterization of absorption of a drug from its formulation.
• Fr=AUCA
AUCB
5. Route Bioavailability (%) Characteristics
Intravenous 100 (by definition) Most rapid onset
(IV)
Intramuscular 75 to ≤ 100 Large volumes often possible;
may be
(IM) painful
Subcutaneous 75 to ≤ 100 Smaller volumes than IM; may
be painful
(SC)
Oral (PO) 5 to < 100 Most convenient; first pass
effects may be
significant
Rectal (PR) 30 to < 100 Less first-pass effects than
oral
Inhalation 5 to < 100 Often very rapid onset
6. • Single dose bioavailability
studies :
are very common. They are easy,
offer less exposure to drugs and are
less tedious.
Limitation:
Difficult to predict the steady-state
characteristics of a drug and inter-
subject variability.
• Multiple dose study :
• the bioavailability is determined at
steady-state.
• Better evaluation of a controlled-
release formulation is possible.
• Small inter-subject variability is
observed,
• Requires collection of fewer blood
samples.
• Limitations:
– Poor compliance by subjects.
– Greater exposure of subjects to
the test drug, increasing the
potential for adverse reactions.
In multiple dose study the drug should
be administered for 5 to 6
elimination half-lives until the
steady-state has been reached,
before collecting the blood samples
➢Single Dose versus Multiple Dose Studies:
dose to be administered for bioavailability study is determined form of
preliminary clinical experiment:
7. • ASSESSMENT OF BIOAVAILABILITY
➢Pharmacokinetics method – This method is more practical and
discriminative. Pharmacokinetic methods are of two types.
a) Determination of whole blood, plasma or serum concentration
b) Urinary excretion method
➢ Pharmacodynamic methods:
• Acute Pharmacologic Response Method : When bioavailability
measurement by pharmacokinetic method is difficult, an acute
pharmacologic effect such as effect on pupil diameter, heart rate or BP can
be useful as an index of drug bioavailability.
• Disadvantage: It tends to be complex, expensive, time-consuming and
require a sensitive and quantitative measure of the desired response.
• Therapeutic Response Method: Clinical response of the drug for which it
is intended to be used is measured.
• E.g.: heart rate, body temperature, blood sugar levels, and for anti-
inflammatory drugs, reduction in inflammation is determined.
• Drawbacks: quantification of observed response is too improper to allow for
reasonable assessment of relative bioavailability between two dosage forms
of the same drug.
8. • A) The blood (or serum or plasma)
concentration-time curve -
• These are based on the assumption that there is a direct relationship
between the concentration of drug in blood or plasma and the
concentration of drug at the site of action.
• If the drugs are given to the volunteers through iv dose, the blood
samples should be withdraw after 5min. And the frequency of sampling
should be 15min.
• In case of one compartment open model – at elimination phase 3 points
are required to describe he kE value.
• In case of two compartmental model – 5 to 6 points are required to
describe kE value.
• If Oral dose is given – 3 points are required to describe ka value.
9. • The key parameters for determining bioavailability
10. AUC: The AUC is proportional to the total amount of drug reaching the
systemic circulation, and thus characterizes the extent of absorption.
Cmax: Gives indication whether drug is sufficiently absorbed systemically to
provide a therapeutic response.
Tmax: The Tmax reflects the rate of drug absorption, and decreases as the
absorption rate increases.
MEC: The minimum plasma concentration of the drug required to achieve a
given pharmacological or therapeutic response
MSC: plasma concentration of the drug beyond which adverse effects are
likely to happen.
11. • THERAPEUTIC RANGE-The range of plasma drug concentration in which
the desired response is achieved yet avoiding adverse effect. The aim is
clinical practice is to maintain plasma drug concentration within the
therapeutic range.
• ONSET OF ACTION-On set of action is the time required to achieve the
minimum effective plasma concentration following administration of drug
formulation.
• DURATION OF ACTION-Duration of action of the therapeutic effect of the
drug is defined as the time period during which the plasma concentration of
the drug exceeds the minimum effective level.
• INTENSITY OF ACTION-In general, the difference between the peak
plasma concentration and the minimum effective plasma concentration
provides a relative measure of the intensity of the therapeutic response of
the drug.
12. B) Urinary Excretion Data:
• These studies are based on the principle that urinary
excretion of the unchanged drug is directly proportional
to the plasma concentration of total drug.
• This technique of studying bioavailability is most useful
for those drugs that are not extensively metabolized
prior to urinary elimination.
13. • The three major parameters examined in urinary excretion
data are as follow:
1.(dXu/dt)max : maximum urinary excretion rate,
gives the rate of appearance of drug in the urine is
proportional to its concentration in systemic circulation. Its
value increases as the rate of and/or extent of absorption
increases
2. (tu)max : time for maximum excretion rate, is
analogous to the of plasma level data, its value decreases
as the absorption rate increases.
3. Xu : cumulative amount of drug excreted in the
urine is related to the AUC of plasma level data and
increases as the extent of absorption increases.
• These studies used for certain thiazide diuretics and
sulfonamides and for drugs that have urine as the site of
action-for example, urinary antiseptics.
15. ● DEFINITIONS
● Equivalence – Equivalence is more relative term that compares
one drug product with another or with a set of established
standards. Equivalence may be defined in several ways:
● Chemical equivalence indicates that two or more dosage forms
contain the labeled quantities of drug.
● Clinical equivalence occurs when the same drug from two or
more dosage forms gives identical in vivo effects as measured
by a pharmacological response or by control of a symptom or a
disease.
● Therapeutic equivalence implies that one structurally different
chemical can yield the same clinical result as another
chemical.
16. The design and conduct of the study should follow ICH
regulations on Good Clinical Practice, including reference to an
Ethics Committee.
A bioequivalence study is basically a comparative bioavailability
study designed to establish equivalence between test and
reference products.
1. Design:
The various types of test designs that are usually employed in
bioequivalence stdies;
i. Completely randomised designs
ii. Randomised block designs
iii. Repeated measures, cross-over and carry-over designs
iv. Latin square designs
17. i. Completely randomised designs
⬜ Method of randomisation
⬜ Label all subjects with the same number of digits, for e.g., if there are 20
subjects, number them from 1 to 20.
⬜ Randomly select non-repeating random numbers (like simple
randomisation) with among these labels for the first treatment, and then
repeat for all other treatments.
⬜ Advantages
⬜ The design is extremely easy to construct.
⬜ It can accommodate any number of treatments and subjects.
⬜ Disadvantages
⬜ Although the design can be used for any number of treatments, it is best
suited for situations in which there are relatively few treatments.
⬜ Any unrelated sources of variability will tend to increase the random error
term, making it difficult to detect differences among the treatment (or
factor level) mean responses.
18. ii. Randomised block designs
⬜ First, subjects are sorted into homogeneous groups, called blocks and the
treatments are then assigned at random within the blocks.
⬜ Method of Randomisation
⬜ Subjects having similar background characteristics are formed as blocks.
⬜ Then treatments are randomised within each block, just like the simple
randomisation.
⬜ Randomisations for different blocks are done independent of each other.
⬜ Advantages
⬜ It can accommodate any number of treatments or replications.
⬜ Different treatments need not have equal sample size.
⬜ The statistical analysis is relatively simple. The design is easy to construct.
⬜ Disadvantages
⬜ Missing observations within a block require more complex analysis.
⬜ The degrees of freedom of experimental error are not as large as with a
completely randomised design.
19. iii. Repeated measures, cross-over and carry-over designs
⬜ This is essentially a randomised block design in which the same subject serves as a
block.
⬜ The administration of two or more treatments one after the other in a specified or
random order to the same group of patients is called a crossover design or
change-over design
⬜ Method of Randomisation
⬜ Complete randomisation is used to randomise the order of treatments for
each subject. Randomisations for different subjects are independent of
each other.
⬜ Advantages
⬜ They provide good precision for comparing treatments because all sources
of variability between subjects are excluded from the experimental error.
⬜ It is economic on subjects. This is particularly important when only a few
subjects can be utilized for the experiments.
⬜ Disadvantages
⬜ There may be an order effect, which is connected with the position in the
treatment order.
⬜ There may be a carry-over effect, which is connected with the preceding
treatment or treatments.
20. iv. Latin square designs
⬜ A Latin square design is a two-factor design (subjects and treatments are the two
factors) with one observation in each cell.
⬜ Such a design is useful to compare the earlier ones when three or more
treatments are to be compared and carry-over effects are balanced.
⬜ In a Latin square design, rows represent subjects, and columns represent
treatments.
⬜ Advantages
⬜ It minimizes the inter-subject variability and carry-over effect in plasma
drug levels.
⬜ Minimizes the variations due to time effect.
⬜ Treatment effects can be studied from a small-scale experiment. This is
particularly helpful in preliminary or pilot studies.
⬜ Disadvantages:
⬜ The randomisation required is somewhat more complex than that for
earlier designs considered.
⬜ The study takes a long time since an appropriate washout period between
two administrations is essential which may be very long if the drug has a
long t½.
21. ⬜ WASHOUT PERIOD
⬜ The time interval between the 2 treatments is
called as WASHOUT PERIOD
⬜ It is required for the elimination of the
administered dose to avoid the carry over effect
⬜ Large no. of drugs have been found to have half –
life between 1-10 hrs, awashout period of 1 week
was usually found suitable in most cases.
22. 2. Subjects:
A. Selection of subjects:
⬜ Aim to minimize variability and permit detection of
differences between pharmaceutical products.
⬜ The studies should normally be performed with healthy
volunteers.
⬜ They should be screened for suitability by means of clinical
laboratory tests, review of medical history, and medical
examination.
B. Standardization of the study:
⬜ The test conditions should be standardized in order to
minimize the variability of all factors involved.
⬜ Standardization of the diet, fluid intake and exercise is
recommended.
⬜ The subjects should not take other medicines during a
suitable period before and during the study.
23. C. Inclusion of patients:
⦿ If the investigated active substance is known to have adverse
effects and the pharmacological effects or risks are considered
unacceptable for healthy volunteers it may be necessary to use
patients instead, under suitable precautions and supervision.
D. Genetic pheno-typing:
⦿ Pheno-typing of subjects should be considered as well in
crossover studies.
⦿ If a drug is known to be subject to major genetic polymorphism,
studies could be performed in panels of subjects of known
phenotype or genotype.
3. Characteristics to be investigated:
⦿ In most cases evaluation of bioavailability and bioequivalence
will be based upon the measured concentrations of the parent
compound.
24. ● In some situations, measurements of an active or inactive
metabolite is carried out.
● The plasma concentration versus time curves are mostly used
to assess extent and rate of absorption.
● The use of urine excretion data may be advantageous in
determining the extent of drug input in case of products
predominately excreted renally.
● Specificity, accuracy and reproducibility of the methods should
be sufficient.
4.Chemical analysis:
● It is conducted according to the applicable principles of Good
Laboratory Practice (GLP).
● Determination of the active moiety and/or its biotransformation
product(s) in plasma, urine or any other suitable matrix must be
well characterized, fully validated and documented to yield
reliable results that can be satisfactorily interpreted.
25. 5 Reference and test product:
• The choice of reference product should be justified by the
applicant and agreed upon by the regulatory authority.
• The test products used in the biostudy must be prepared in
accordance with GMP-regulations.
6.Data analysis:
• To quantify the difference in bioavailability between the
reference and test products and to demonstrate that any
clinically important difference.
A.Statistical analysis:
• The statistical analysis (e.g. ANOVA) should take into
account sources of variation that can be reasonably assumed
to have an effect on the response variable.
• Pharmacokinetic parameters derived from measures of
concentration, e.g. AUC, Cmax should be analyzed using
ANOVA.
26. B. Acceptance range for pharmacokinetic parameters:
1.AUC-ratio:
● It should lie within an acceptance interval of 0.80-1.25.
2.Cmax-ratio:
● It should lie within an acceptance interval of 0.80-1.25.
● The wider interval must be 0.75-1.33.
➢ For tmax if there is a clinically relevant claim for rapid release
or action or signs related to adverse effects. The interval
should lie within a clinically determined range.
C. Handling deviations from the study plan:
● The protocol should also specify methods for handling drop-
outs.
D.A remark on individual and population bioequivalence:
● Bioequivalence studies are designed for population and
individual is limited.
27. 7.In vitro dissolution for bioequivalence study:
✕ The term commonly used to describe is "in-vitro/in-vivo
correlation".
✕ The specifications for the in vitro dissolution of the product
should be derived from the dissolution profile of the batch.
A. Official dissolution tests:
✕ Apparatus 1, (basket method).
✕ Apparatus 2 (paddle method).
B.Parameters used:
1. Degree of agitation
2. Size and shape of container
3. Composition of dissolution medium
• pH, ionic strength, viscosity
4. Temperature of dissolution medium
5. Volume of dissolution medium
28. 8.Reporting of results:
● The report of a bioequivalence study should give the
complete documentation of its protocol, conduct and
evaluation complying with GCP-rules and ICH guideline.
● Drop-out and withdrawal of subjects should be fully
documented.
● The method used to derive the pharmacokinetic
parameters should be specified.
● The analytical report should include the results for all
standard and quality control samples.
29. APPLICATIONS FOR PRODUCTS CONTAINING
APPROVED ACTIVE SUBSTANCES:
A. Bioequivalence studies:
⦿ In vivo bioequivalence studies are needed when there is
a risk that possible differences in bioavailability may
result in therapeutic in equivalence.
⦿ oral immediate release drug formulations with systemic
action
⦿ Non-oral and non-parenteral drug formulation designed
to act by systemic absorption.
⦿ Sustained or otherwise modified release drug
formulation.
⦿ Fixed-dose combination products.
30. ● REFERENCES:
● Brahmankar.D.M,Sunil.B.Jaiswal,Vallabh Prakashan
Biopharmaceutics and Pharmacokinetics-A Treatise
,page no.282-305.
● LeonShargel & Andrew Yu Applied Biopharmaceutics &
pharmacokinetics, page no 247-260.
● Madan.PL Biopharmaceutics & pharmacokinetics page
no 118-127.
●