2. INTERVENTIONAL RADIOLOGY IN LT 331
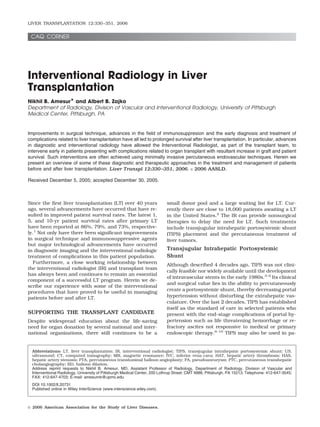
tients with Budd Chiari Syndrome who are either not LT 12-34%).41 In rare cases, severe uncontrolled hepatic
candidates or awaiting LT.11 Long-term patency issues encephalopathy or hepatic insufficiency may ensue.
with TIPS requiring secondary interventions to main- Here again the IR may be called upon to reduce the
tain flow has lead to the general opinion that patients flow through the TIPS or even occlude it if necessary
who are in Child-Turcotte-Pugh class A should undergo (Fig. 1).42,43
shunt surgery while patients in Child-Turcotte-Pugh
classes B and C are better suited for TIPS.12 Percutaneous Treatment of Liver Cancers
Absolute contraindications to TIPS include: elevated
central venous pressures from right heart failure, se- The best treatment results for hepatocellular carci-
vere hepatic failure, severe encephalopathy, active in- noma and other primary liver malignancies may be
fection, and advanced polycystic liver disease. Relative achieved from local surgical resection or liver trans-
contraindications that can make the procedure chal- plantation. Whereas LT may offer the best treatment for
lenging but possible in experienced hands include por- patients who are not candidates for local resection, the
tal vein thrombosis and hepatic neoplasms.13-15 availability of organs is limited.44-47 Long waiting times
As experience with this procedure16-18 and its com- for LT may result in progression of their disease even to
plications19,20 has grown, we have learned that TIPS is the point of risking their candidacy.48,49 Established
not a cure for portal hypertension but often serves well transplant criteria for hepatocellular carcinoma usu-
as a bridge to LT. Intractable ascites21-23 and resistant ally includes patients with a single lesion less than 5 cm
variceal bleeding24 can often be satisfactorily managed in diameter or up to 3 tumors, none exceeding 3 cm in
with TIPS placement while awaiting LT. Although TIPS diameter.50,51 Percutaneous local ablative therapies
is effective in many patients, several prognosticators such as transarterial chemoembolization, radiofre-
have been developed that predict poor patient survival quency ablation, and percutaneous ethanol ablation
and increased mortality rates after TIPS. These include therapies may be employed to control tumor progres-
advanced liver disease associated with elevations in sion while awaiting LT as well as to help increase post-
serum bilirubin, international normalized ratio, and se- transplantation survival rates.52-56 Furthermore, there
rum creatinine.25-30 is data indicating that patients with lesions larger than
The technique of TIPS placement has been well de- 5 cm may achieve longer-term survival after LT in the
scribed31-33 and will not be described here. A baseline context of multimodal adjuvant therapy.57
ultrasound (US) is obtained within 24 hours of TIPS
placement. The baseline US should be delayed by at THE ROLE OF RADIOLOGY IN
least 3 days if a covered stent is used, since it may take PREOPERATIVE AND DIAGNOSTIC
2-3 days for the air in the graft material to be replaced
with fluid and allow transmission of US. Serial US ex-
EVALUATION
aminations can be performed initially at 3-month inter- Routine preoperative visceral angiography has largely
vals or based on institutional protocol. been replaced by noninvasive studies such as US, com-
Pseudointimal hyperplasia, usually at the hepatic ve- puted tomography (CT), and magnetic resonance (MR)
nous end, results in narrowing and eventually occlu- imaging.58-64
sion of the TIPS. Biliary leak from transection of bile Newer generation helical CT scanners provide out-
ducts during TIPS placement is a known cause of early standing quality images. Abdominal CT has a much
TIPS thrombosis and may be avoided by the use of better detection rate for hepatic mass lesions, espe-
covered stents.34 Primary patency rates of TIPS are cially when a helical CT scan is performed with arte-
reported to range from 20 to 69%.12,35-37 Surveillance rial and venous phase imaging.65 Powerful worksta-
US can help identify narrowing within the TIPS and tions, in conjunction with newer generation
early reintervention with balloon angioplasty and/or multidetector CT scanners, allows the rapid creation
restenting can prolong the life of the TIPS resulting in of 3-dimenisional angiographic quality images in a
assisted secondary patency rates approaching 90%. short time period. This is particularly important in
Recent studies indicate that the use of covered stents accurately evaluating vascular anatomy.66-70 In liv-
may be associated with fewer reinterventions with pri- ing donor transplantation, there is a tremendous
mary 1-yr patency rates reported at 80%.38-40 pressure for minimizing invasive procedures in the
Complications from TIPS can vary across a vast spec- donor without sacrificing preoperative accuracy.71
trum. Procedure related death rates are reported to be Sakai et al.72 found that, at contrast infusion rates of
less than 2%, and usually linked to laceration of vessels 4 mL/second, there was higher visualization of the
involved in the creation of the TIPS.41 Mortality rates in smaller visceral branches and they successfully iden-
the first 30 days are reported at an average of 11% and tified 23 of 24 aberrant vessels.
is related to liver failure, acute respiratory distress syn- Even though previous studies have demonstrated US
drome, sepsis, recurrent hemorrhage, or right heart or to be relatively insensitive in the detection of malig-
multiorgan failure.12 A successful TIPS can control nancy in end-stage cirrhotic livers,73 newer generation
acute hemorrhage in greater than 90% of patients and scanners and the use of contrast agents have greatly
provide relief from recurrence of variceal bleeding in improved detection rates.74 US also can be performed
about 80% of patients. Encephalopathy is reported in relatively quickly at the bedside, making it more appeal-
up to a third of patients following TIPS (range ing in the often critically ill perioperative patient. Pa-
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
3. 332 AMESUR AND ZAJKO
Figure 1. (A) Patient with florid liver failure post TIPS
treated by occluding the TIPS with large coils placed
through a balloon occlusion catheter. (B) Complete occlusion
of the TIPS after placement of multiple coils. (C) Another
patient with liver failure was treated by placing a con-
strained Wallstent placed within the old TIPS to reduce flow.
tency and flow directionality can be adequately demon- patients severely allergic to iodinated contrast agents or
strated at the bedside.75 Newer techniques utilizing US with renal insufficiency.
contrast agents and microbubbles may yield better di- Surgeon preference and strengths of individual ra-
agnostic rates.76-78 diology departments still plays an important role in
Advancements in MR imaging and MR angiography determining which study is performed. When clini-
pulse sequences and the use of contrast agents have cally indicated, our surgeons still request catheter-
laid the foundation for this modality to be safely and based angiograms on living liver donors. Despite ad-
effectively used in the LT population.79-82 In fact, the vances in CT and MR imaging conventional catheter-
ability of a noninvasive study to provide multiplanar based diagnostic angiography is still performed in
anatomic, vascular, and cholangiographic data is very select cases. One such area is portal vein occlusion
appealing, especially in the living donor popula- seen on CT. Selective superior mesenteric artery ar-
tion.83,84 Three-dimensional gadolinium-enhanced MR teriography with portal vein imaging can demonstrate
angiography also plays a role in the evaluation of com- the condition of the superior mesenteric vein, which
plications in the posttransplantation patient.85 Addi- can be used as a site for portal vein allograft anasto-
tionally, MR imaging and US can safely be used in mosis using an interposition venous graft.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
4. INTERVENTIONAL RADIOLOGY IN LT 333
Figure 2. (A) No flow into the hepatic artery post OLTX is
seen on celiac arteriogram. Note filling of some small collat-
eral vessels near the hilum of the liver. (B) Irregular appear-
ing biliary dilation seen on CT. (C) Biliary necrosis seen on
catheter cholangiography post biliary drainage catheter
placement.
Normal Vascular and Biliary Reconstructions to the recipient’s infrarenal aorta or, in rare cases, other
areas such as the suprarenal abdominal aorta,87 the
A successful LT requires at least 1 arterial, 2 venous, splenic artery,88 and even the inferior epigastric ar-
and 1 biliary anastomosis. More than 75% of livers tery.89 It is important for the IR to be aware of these
derive their entire arterial supply from the celiac axis, various anastomoses both for diagnostic and interven-
allowing the creation of a single arterial anastomosis.86 tional purposes.90-92
In the case of aberrant hepatic vasculature, complex A direct end-to-end portal anastomosis is usually
arterial anastomoses may need to be created on the
performed. In the case of portal vein thrombosis, a
operating room table.
surgical thrombectomy may be needed or an interposi-
The Carrell patch is the arterial anastomosis of
tion graft may be utilized from the recipient superior
choice. Here the donor celiac trunk is preserved with a
mesenteric vein.93
small segment of the surrounding donor aorta and
anastomosed to the recipient common hepatic artery. Two common hepatic venous reconstructions are uti-
This is usually followed by ligation of the donor splenic, lized. A piece of the donor intrahepatic inferior vena
left gastric, and gastroduodenal arteries. However, cava (IVC) with the attached native hepatic veins may
sometimes these vascular stumps are used as anasto- be interposed into the recipient’s IVC, creating a supra-
motic sites for on-table attachment of accessory ves- hepatic and infrahepatic anastomosis. An alternate
sels, such as a variant right hepatic artery from the anastomosis is the “piggyback” anastomosis. This is
superior mesenteric artery. created by suturing together the hepatic veins to form a
In retransplantation, or in cases in which a success- cloaca, which is then directly anastomosed to the donor
ful attachment to the recipient cannot be performed suprahepatic IVC with ligation of the donor infrahepatic
(e.g., celiac axis stenosis, short donor hepatic artery), a IVC.
donor iliac artery interposition homograft or, rarely, a The choledochocholedochostomy and the Roux-en-Y
prosthetic graft may be utilized. These may be attached choledochojejunostomy are the 2 main biliary recon-
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
5. 334 AMESUR AND ZAJKO
Figure 3. (A) No filling of the hepatic artery seen on celiac arteriogram. (B) Revascularization was done via an anastomosis to an
hepatic branch from the SMA. Note kink and stenosis of the HA. Because the patient was three days postoperative from the
transplant, this was treated surgically.
structions utilized.94,95 The choledochocholedochos- than conventional percutaneous biopsy.100-103 Fur-
tomy is an end-to-end anastomosis between the donor thermore, it allows the IR to obtain wedged hepatic
and recipient common bile ducts. Alternate anastomo- venous pressures if there is clinical concern for portal
ses include a choledochojejunostomy or a hepaticojeju- hypertension.
nostomy to a Roux-en-Y loop of jejunum.
POSTOPERATIVE INTERVENTIONS
DIAGNOSTIC INTERVENTIONS
Postoperative complications may occur in up to 25% of LT
Percutaneous Liver Biopsy recipients.104-108 Any decline in liver function should
Image-guided, directed, and random liver biopsies are prompt an early search for a potentially reversible cause.
often called upon in the LT patient population.96 Argu- US provides a noninvasive and portable means of quickly
ments against image-guided liver biopsy are made for evaluating the vascular flow within the allograft as well
cost effectiveness and whether they add to the diagnos- as evaluating for intrahepatic biliary dilation. At the
tic yield of the procedure in the non-LT patient.97-99 same time US also provides a safe means of perform-
However, imaging with US and in some cases CT allows ing a percutaneous liver biopsy at the bedside, if
visualization of other abnormalities such as ascites and required. CT and MR imaging also provide noninva-
vascular structures that can be avoided, thereby reduc- sive evaluation of the transplanted liver.109 Not only
ing complication rates. In patients with split-liver can vascular and biliary complications be easily iden-
transplants, image guidance is required to safely per- tified, but postoperative fluid collections can be dem-
form the biopsy and avoid entering the bowel or other onstrated. Three-dimensional reformats often pro-
adjacent organs. In cases of extensive ascites, percuta- vide diagnostic angiography quality images.110
neous liver biopsy is avoided due to the higher risk of Arterial Complications
peritoneal bleed. If a directed biopsy is needed, a drain-
age catheter can be placed into the ascites prior to the Hepatic artery stenosis and especially hepatic artery
biopsy. thrombosis (HAT) may result in arterial insufficiency to
the LT.
Transjugular Liver Biopsy
Hepatic Artery Thrombosis
Indications for random transjugular liver biopsy in-
clude the need for a nondirected biopsy in patients HAT rates in the LT recipient range from 4 to 42% with
with coagulopathy, thrombocytopenia, or massive as- the higher rates seen in the pediatric population, in
cites. In such cases, transjugular liver biopsy has which complex, technically demanding anastomoses
been shown to yield adequate tissue with a high di- are created on much smaller vessels.111-117 Risk fac-
agnostic yield and a lower bleeding complication rate tors linked to HAT include increased cold ischemia
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
6. INTERVENTIONAL RADIOLOGY IN LT 335
Figure 4. (A) Severe hepatic artery stenosis seen on celiac
arteriogram. (B) Balloon angioplasty was performed using a
5mm balloon. (C) Excellent angiographic result seen post
angioplasty.
time, ABO blood group incompatibility, small donor asymptomatic patients vs. 65% in the symptomatic pa-
vessels, rejection, arterial kinks, and reduced flow sec- tients.
ondary to hepatic artery stenosis (HAS).104 Ishigami et The hepatic artery provides the only vascular supply
al.118 also reported a higher risk of hepatic arterial to the biliary tract epithelial lining of the allo-
complications in patients with variant hepatic artery graft.122,123 Thus HAT is usually associated with biliary
anatomy. ischemia and resultant strictures,124,125 necrosis,
Mortality rates from HAT have been reported to be leaks with biloma formation, and intrahepatic ab-
greater than 80% without emergent retransplantation scesses (Fig. 2).
or revascularization.119,120 Sheiner et al.121 reported US offers a relatively inexpensive, portable, noninva-
that out of 1,026 liver transplantations at their institu- sive, and readily available method of evaluating the liver
tion, 32 patients (3.1%) developed HAT. Of these, only parenchyma and hepatic arterial flow.126-129 Flint et
20 (62.5%) were symptomatic. However, they found al.130 correctly identified 92% of HAT by Doppler US
that graft salvage in asymptomatic patients undergoing examination. The resistive index and systolic accelera-
revascularization was 82% vs. 40% in symptomatic pa- tion times can be calculated from the Doppler waveform
tients resulting in a 1-yr patient survival of 92% in seen in the transplant hepatic artery. A resistive index
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
7. 336 AMESUR AND ZAJKO
Figure 5. (A) Severe HA stenosis seen on CTA. (B) The stenosis is confirmed on celiac arteriography. (C) Balloon angioplasty
performed. (D) Improved flow and caliber of the vessel is seen post angioplasty.
of less than 0.5 or systolic acceleration times of greater be hard to differentiate from HAT on US, but needs to be
than 0.08 seconds is highly suggestive of stenosis or aggressively looked for, since HAS may be a treatable
thrombosis of the vessel.131 complication and prolong the life of the allograft. Cath-
Three-dimensional helical CT arteriography with eter-based arteriography is usually performed at our
maximum intensity projection and shaded surface dis- institution to confirm and treat HAS.
play techniques offers a noninvasive approach to the Prior to arteriography it is vital that the IR be fully
diagnosis of vascular complications after LT. A sensi- aware of the surgical vascular anastomoses that were
tivity rate of 100% with a 89% specificity and accuracy utilized in the patient. If a standard Carrell patch was
of 95% has been demonstrated.110 utilized we usually begin with a celiac arteriogram.
Initial experience with implantable Doppler probes at Standard angiographic catheters such as a Cobra
the time of LT for continuous blood flow monitoring for (Cook Incorporated, Bloomington, IN) or Sos (Angiody-
a short time period after LT has also been described and namics, Queensbury, NY) are utilized since they can be
may be beneficial.132 gently placed in the origin of the celiac trunk without
Once an abnormal US and/or CT result is obtained, the guidewire needing to be advanced across the anas-
an arteriogram is usually performed. Severe HAS may tomosis. This is important since it may be difficult to
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
8. INTERVENTIONAL RADIOLOGY IN LT 337
Figure 6. (A) Large pseudoaneurysm arising from a branch
of the right hepatic artery is demonstrated on common he-
patic arteriogram. (B) In preparation for embolization, the
pseudoaneurysm is catheterized with a microcatheter. (C)
After the PA is filled with microcoils, post embolization ar-
teriography shows occlusion of the PA.
differentiate guidewire associated spasm/dissection vs. gent surgical intervention may be needed for cases in
stenosis/occlusion. which percutaneous techniques fail to improve flow.137
In cases of an infrarenal graft, we initially perform a
lateral abdominal aortogram with an aortic flush cath-
eter. This allows adequate delineation of the graft origin
Hepatic Artery Stenosis
and can be followed by selective graft catheterization to HAS rates as high as 11% have been re-
define the intrahepatic vasculature and identify de- ported.107,108,138,139 Early recognition and interven-
layed filling of intrahepatic branches via collaterals. tion may help prevent significant ischemic organ
Sometimes a variant anastomosis may be in place and damage and progression to HAT.140 The vast majority
could be missed if the operative note is not reviewed. of HAS occurs at the surgical anastomosis and is
Although many potential collateral pathways are sev- linked to technical factors, clamp injury, kinked ves-
ered during LT, extensive extrahepatic arterial collater- sels, fibrosis, edema, and thrombus formation. Non-
als may form in the posttransplantation patient follow- anastomotic stenoses may be secondary to allograft
ing HAT. If such collateral pathways are identified and rejection or clamp injury. A redundant hepatic artery
the occlusion is believed to be acute, endovascular re- with kinks can simulate HAS both physiologically
vascularization techniques may be pursued. and angiographically and may be best managed sur-
There are many reports of restoration of flow with gically. Immediate postoperative HAS is most likely
catheter directed thrombolytic therapy and mechanical related to surgical technique and is also best man-
thrombectomy devices.133-136 Once the thrombus is aged surgically. Early postoperative PTA may lead to
cleared an underlying stenosis may be uncovered and vascular rupture (Fig. 3). We have pursued PTA as
can then be treated with percutaneous transluminal early as 10 days after LT at our institution.
balloon angioplasty (PTA) and/or stent placement. Ur- Initial reports of PTA were based on older balloon
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
9. 338 AMESUR AND ZAJKO
Figure 7. (A) Stenosis of the MPV at the surgical anastomosis is demonstrated on US. (B) Severe anastomotic stenosis is
demonstrated on portal venogram performed via the transhepatic approach. (C) Note the waist in the mid portion of the 16mm
angioplasty balloon. (D) Note obliteration of the balloon waist upon further dilation to maximum pressure. (E) Minimal residual
stenosis at the surgical anastomosis is seen on final post angioplasty venography.
technology in which 5-French (Fr) balloon catheters Many of these patients have liver dysfunction with
were utilized over 0.035-inch guide wires. This made resultant coagulopathy. The development of percutane-
balloon angioplasty within tortuous vessels cumber- ous femoral artery closure devices and pads allow per-
some and sometimes impossible. Advancements in bal- cutaneous access site hemostasis in the face of poor
loon technology have resulted in lower profile balloons coagulation with ease though they are not completely
that can easily track around curves, often seen in the free of complications.141-147
LT patient. Many of these balloons can be used over Data on liver function recovery after PTA are scant,
thin 0.014 inch and 0.018 inch guidewires that can be but several small series indicate allograft func-
placed through 5 Fr low profile guiding sheaths posi- tion may improve with the timely performance of
tioned at the origin of the celiac axis (Figs. 4 and 5). The PTA for HAS.140,148-150 Previous data from our insti-
guiding sheaths allow easy exchange of catheters and tution151 showed significant improvement in mean
the ability to inject contrast material around the bal- aspartate aminotransferase and alanine aminotrans-
loon. Additionally, if PTA is unsuccessful or is compli- ferase levels within 1 week after successful PTA.
cated by a dissection, lower profile stent delivery sys- However, severe initial allograft dysfunction is a
tems designed to be placed over 0.018 inch guide wires poor prognostic sign and is often associated with
can be placed through the guiding sheath. Unfortu- allograft loss and the eventual need for retransplan-
nately, the presence of stents may complicate retrans- tation, regardless of the success or failure with
plantation, but if needed extraanatomic bypass grafts PTA.152
can be used. PTA and stent placement can be a safe procedure in
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
10. INTERVENTIONAL RADIOLOGY IN LT 339
Figure 8. (A) Transhepatic portal venogram demonstrates
recurrent narrowing in a patient who underwent previous
portal vein angioplasty. Note the presence of embolization
coils that were used to seal the previous angioplasty tract.
(B) Patient was treated with a metal stent. (C) Improved
portal venous flow seen after stent placement.
experienced hands but is also fraught with complica- commonly seen arterial complications post-LT (Fig.
tions, including spasm,153 dissection, occlusion, and 6).156 These may be due to surgical anastomotic break-
pseudoaneurysm154,155 formation. down from technical factors or infection157 or may be
related to posttransplantation iatrogenic injuries
Hepatic Artery Graft such as from balloon angioplasty, percutaneous bili-
ary drainage,158,159 or biopsy. The diagnosis of PA
Both stenosis and thrombosis of the hepatic artery graft
can usually be made by noninvasive imaging such as
can be seen and are treated no differently than HAS or
HAT. In cases of graft stenosis they may occur at the US or CT.160 Since the PA may rupture, they must be
proximal or distal anastomosis. repaired to avoid potentially serious complications
such as hemoperitoneum, hemobilia, or massive gas-
trointestinal tract bleeding.161 Traditional treat-
Hepatic Artery Pseudoaneurysm ments for such abnormalities have relied on surgical
Hepatic artery pseudoaneurysm (PA) formation and ar- exploration and resection.162 Percutaneous endovas-
teriovenous fistula represent some of the other less cular treatments may be employed to treat some of
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
11. 340 AMESUR AND ZAJKO
Figure 9. (A) Severe IVC anastomotic stenosis seen on vena cavography in a patient post OLTX. (B) Due to large size of the IVC,
three balloons were inflated simultaneously across the stenosis. (C) Normal anastomosis seen post angioplasty.
these complications. Transvascular coil embolization lowed by PTA. On average, large-sized balloons in the
may be performed if there is an adequate neck to the order of 10 to 16 mm may be needed to treat main portal
PA or if the arteriovenous fistula can be catheterized. vein stenosis in adult LT recipients (Fig. 7). Unsuccess-
Newer technology detachable coils such as the NXT ful PTA or recurrent stenosis can be treated with stent
(Micro Therapeutics, Irvine, CA) developed for neuro- placement (Fig. 8). Once the treatment is completed the
vascular procedures may play a role in occluding intraparenchymal tract can be embolized with coils or
more complex aneurysms. These coils are placed into gelfoam to prevent any bleeding into the peritoneal
the aneurysm through microcatheters. Once they are space. If a large amount of ascites is present, it should
in position and felt to adequately fill the space needed be drained prior to access.
and are stable, they can be released by a low voltage
There have been several reports of successful treatment
electric charge through the attachment wire. If the IR
of portal vein stenosis using PTA and stents when need-
is not satisfied with coil placement or if the distal flow
ed.171-174 Funaki et al.175 successfully treated 19 of 25
is compromised it can simply be withdrawn without
pediatric LT patients with percutaneous techniques.
detachment. Occasionally, if there is extreme tortu-
osity of the vessels, direct percutaneous access Twelve patients needed to be stented with patency main-
may be utilized for embolization or thrombin injection tained at 46 month mean follow-up. Surgical thrombec-
into the PA.163 As stent technology improves, low tomy and placement of intraoperative stent placement
profile covered stent grafts can be placed to occlude a has been reported.176 The treatment of portal vein thromb-
PA or the venous communication in an arteriovenous osis by percutaneous transhepatic portal vein thrombo-
fistula.164,165 lysis and stent placement if needed as well as via a trans-
jugular approach has been described.177-180
Portal Vein Complications
Portal vein stenosis may be seen in less than 3% of Inferior Vena Cava and Hepatic Venous
adult LT recipients and rates of 7% have been re-
Complications
ported in the pediatric population, with some pro-
gressing to portal vein thrombosis.166,167 Most occur at IVC stenosis or thrombosis is seen in less than 1% of LT
the surgical anastomosis and may be related to surgical recipients.181 They mostly occur at the surgical anasto-
technique, a redundant vein, or the use of a bypass mosis or less often, are due to extrinsic compression and
graft. Patients may be asymptomatic or present with
mass effect from surrounding fluid collections or hema-
the clinical signs of portal hypertension. Portal vein
toma formation. Suprahepatic IVC stenosis may present
thrombosis generally presents with elevation of liver
with ascites and pleural effusions with a Budd-Chiari-like
enzyme levels as well as signs of portal hypertension
syndrome. Infrahepatic stenoses may present with lower
such as variceal bleeding, ascites, or splenomegaly.
Noninvasive imaging usually demonstrates the stenosis body edema due to poor venous return. The incidence of
and any associated thrombus.168 Direct venography is upper and lower caval anastomotic stenosis is approxi-
usually performed to confirm the diagnosis and to treat mately equal.182 Endovascular techniques can help alle-
the complication. The portal vein can be accessed via a viate these problems. PTA, stent placement, and throm-
transhepatic, transjugular, or even a transsplenic ap- bolysis can provide minimally invasive methods of
proach.169,170 At our institution we prefer the transhe- treating these patients.183,184 Despite the current avail-
patic approach. After gaining transhepatic access, a ability of large-sized balloons, single balloons may not be
5-Fr diagnostic catheter can be placed into the splenic large enough to dilate the IVC. Simultaneous inflation of
or superior mesenteric vein for portal venography fol- multiple balloons has been described in these cases (Fig.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
12. INTERVENTIONAL RADIOLOGY IN LT 341
Figure 10. (A) Severe central right hepatic stenosis is seen
on selective hepatic venography. Note that some contrast
material enters the inferior vena cava and demonstrates an
IVC stenosis as well. Note the collateral veins arising from
the hepatic vein at multiple locations. (B) Simultaneous bal-
loon dilation of the right hepatic vein and IVC was per-
formed. (C) Improved patency and flow through the hepatic
vein and IVC is seen on post angiography venography. Note
the absence of filling of the collateral veins.
9). Resistant stenoses or those with elastic recoil may Biliary Intervention
need to be treated with large stents.185,186
Biliary tract complications post-LT were once reported
Hepatic venous stenosis may be seen in 4 to 5% of
post-LT patients.187 The higher numbers are often seen to be as high as 48%, with more recent reviews indicat-
in partial LT. On US they show flattened monophasic ing a 10 to 15% range.189-195 The choledochochole-
flow with decreased velocities of less than 10 cm/sec- dochostomy and the Roux-en-Y choledochojejunos-
ond.188 They can present with vascular engorgement tomy are the 2 preferred biliary reconstructions
and biopsy results that indicate passive liver conges- utilized.196 Biliary obstruction and leaks are the 2 ma-
tion. PTA is once again the first line of treatment (Fig. jor groups of LT complications that often require inter-
10). A jugular approach is preferred in patients with a vention. An endoscopic approach may be difficult with
piggyback anastomosis as it is easier to access. Stent the presence of Roux-en-Y loops.197 The IR may be
placement can be problematic since they often have to called upon to perform diagnostic percutaneous trans-
be extended into the IVC but can be pursued if needed hepatic cholangiography (PTC) followed by drainage or
(Fig. 11). intervention. Anastomotic strictures are usually related
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
13. 342 AMESUR AND ZAJKO
Figure 11. (A) Severe right hepatic venous stenosis is shown on a right hepatic venogram performed from a right internal jugular
vein approach several months post transplantation. (B) During balloon angioplasty, a moderate waist is seen in the balloon lumen
at maximum inflation pressure. (C) Residual stenosis is seen post balloon dilation. (D) An endovascular metal stent was placed
across the stenotic vein resulting in a wide open hepatic vein.
to scar tissue and technical factors. Nonanastomotic bility of biliary necrosis. Percutaneous interventional
strictures may be related to hepatic arterial insuffi- techniques, especially with HAS, may be safely used to
ciency, infection, ABO blood group incompatibility, and treat many of these complications.204-206
primary sclerosing cholangitis.198-201 The arterial sup- Until fairly recently, CT and US have provided the
ply to the biliary tree is derived from the right and left only noninvasive means of detecting postoperative bil-
hepatic arteries that form a plexus of blood vessels iary complications. Previous data from our institu-
around the right and left ducts that continue into the tion207 has shown that US can miss biliary tract abnor-
common duct.202,203 In the post-LT patient, collateral malities after LT. However, newer generation scanners
supply to the liver is poor, thus any situation such as in the hands of experienced ultrasonographers can eas-
HAS or HAT may result in biliary ischemia with result- ily identify biliary abnormalities.74
ant strictures and obstruction with the eventual possi- The rapid evolution of MR techniques and contrast
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
14. INTERVENTIONAL RADIOLOGY IN LT 343
Figure 12. (A) The left lobe biliary tree is pacified by transhepatic cholangiography in a patient status post OLTX. Note the
extensive irregular bile ducts filled with debris. (B) After percutaneous drainage, catheter cholangiography demonstrates diffuse
irregular beaded appearance of the biliary tree compatible with recurrent primary sclerosing cholangitis fifteen years after liver
transplantation.
agents have allowed the creation of MR cholangiopan- Mild narrowing at the surgical anastomosis may be
creatography images that can provide details that were secondary to ductal size mismatch and should be dif-
once only appreciated with PTC.208-210 ferentiated by free drainage into the small bowel. If
during PTC the intrahepatic ducts are dilated despite
some drainage into the small bowel, an empiric trial of
Percutaneous Transhepatic Cholangiography
biliary catheter drainage may be pursued to look for
and Drainage improvement in liver enzyme levels. If liver function
PTC is still relied on in questionable cases at our insti- improves after biliary drainage and a focal lesion is
tution. It also allows the prompt drainage of dilated identified on follow-up cholangiography, percutaneous
ducts for biliary decompression. The technique is rela- treatment with balloon dilation (BD) can be pursued
tively simple in principle but may be difficult and will (Fig. 13). At our institution we usually perform up to 3
not be described in detail here. sets of serial BDs spread over 1 to 2 weeks for a total of
If after a diagnostic PTC, a guidewire cannot be easily 30 minutes of balloon inflation per session. A drainage
advanced through the obstruction, an external drain- catheter is left in place across the narrowing and the
age catheter is placed to allow biliary decompression. patient returns after several weeks for a follow-up chol-
Extensive initial manipulation can result in the rapid angiogram. If satisfactory results are seen, the catheter
onset of sepsis and should not be pursued. After the can be removed or the trial extended by placing the
biliary tract has drained for a couple of days, advance- catheter above the site of BD. Surgical revision may be
ment through the obstruction can be reattempted with pursued in those patients who do not respond to per-
increased chance of success and decreased risk of sep- cutaneous BD. Chronic catheters may be left in place in
sis. patients who are poor surgical candidates; such cath-
eters may be need to be changed every 6 to 12 weeks as
tolerated.
Bile Duct Obstruction Previous published reports from our institution dem-
Strictures are the most common cause of biliary ob- onstrate 80% patency at 6 months, decreasing to 60%
struction. Anastomotic strictures are often related to at 5 years in 72 patients.216 Generally higher rates of
scarring and fibrosis at the surgical anastomosis. Non- surgical intervention are needed in the pediatric popu-
anastomotic strictures can result from prolonged cold lation. The presence of a Roux-en-Y loop makes endo-
ischemia, vascular insufficiency from HAS, or HAS, and scopic retrograde cholangiopancreatography nearly im-
is also linked to cytomegalovirus infection.211-213 Stric- possible. Percutaneous BD of strictures has been
tures may also be secondary to recurrence of primary successfully described in the pediatric and living re-
biliary tract lesions such as from cholangiocarci- lated liver donor transplantation.217,218 In fact, Lorenz
noma214 and primary sclerosing cholangitis (Fig. 12).215 et al.217 recently described 58% patency of biliary-en-
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
15. 344 AMESUR AND ZAJKO
Figure 13. (A) Severe stenosis of the hepatic jejunostomy
anastomosis seen on PTC. (B) Percutaneous balloon dilation
was performed. (C) Marked improvement seen at the anasto-
mosis post balloon dilation on catheter cholangiogram.
teric anastomosis 1 yr after BD. Higher patency rates the so-called “cutting balloons,” have been used to treat
may be achieved after BD in patients with patent he- resistant biliary strictures with some success. Further
patic arteries.219 work in this area may prove these balloons to be more
Newer balloons with attached microsurgical blades, superior than standard high pressure balloons alone;
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
16. INTERVENTIONAL RADIOLOGY IN LT 345
however, the risks of biliary leaks has not been estab- CONCLUSION
lished.220
Advances in the field of percutaneous endovascular
Percutaneous metallic stent placement for failed bal-
techniques have progressively increased the impor-
loon dilation of benign strictures has been described
tance of the IR in the management of LT patients. The IR
previously.221,222 Culp et al.223 described the place-
should be considered a vital member of the transplan-
ment of 61 metallic stents in 36 LT recipients resistant
tation team, immediately available for consultation,
to BD. Their primary patency was 44% at 3 years and
who can help manage pre- and postoperative problems
0% at 5 years; secondary patency with reintervention
often seen exclusively in this patient population. The
resulted in 88% patency at 5 years. The presence of
timely and judicious use of percutaneous diagnostic
metallic stents in the biliary tree may also pose a tech-
and interventional procedures can help decrease pa-
nical challenge for future retransplantation. The use of
tient morbidity and mortality, increase graft survival,
temporary, retrievable, covered stent grafts in the bili-
and preserve or improve allograft function.
ary tree for such resistant stenosis has been reported
but with 50% restenosis rates at 6 months.224 However,
as stent graft technology improves, this avenue may REFERENCES
prove to be of further value.
Malfunctioning T-tubes or indwelling surgically 1. Organ Procurement and Transplantation Network.
http://optn.org. Accessed: July 29, 2005.
placed plastic stents can also contribute to biliary ob-
2. Organ Procurement and Transplantation Network.
struction. Once the suture is resorbed, the plastic http://optn.org. Accessed: September 23, 2005.
stents usually migrate into the bowel and are excreted. 3. Richter GM, Palmaz JC, Noeldge G, et al. The transjugu-
An occluded stent may lodge at the anastomosis or even lar intrahepatic portosystemic stent-shunt: a new non-
the cystic duct remnant, resulting in biliary obstruc- surgical percutaneous method. Radiologe 1989;29:406-
tion. Such stents may be snared percutaneously or 411.
endoscopically. 4. Richter GM, Noeldge G, Palmaz JC, et al. Transjugular
intrahepatic portocaval stent shunt: preliminary clinical
Biliary stones can sometimes be missed during LT or
results. Radiology 1990;174:1027-1030.
form subsequently, leading to biliary obstruction. The
5. Kauffmann GW, Richter GM. Transjugular intrahepatic
prevalence of bile duct filling defects post-LT has been portosystemic stent-shunt (TIPSS): technique and indica-
reported to be 5.7% from our institution.225 A total of tions. Eur Radiol 1999;9:685-692.
34% represented stones, 56% were sludge or biliary 6. Boyer TD, Haskal ZJ. American Association for the Study
cast, and 10% were necrotic debris. Endoscopic retro- of Liver Diseases Practice Guidelines: the role of tran-
grade cholangiopancreatography may be difficult or im- sjugular intrahepatic portosystemic shunt creation in the
management of portal hypertension. J Vasc Interv Radiol
possible to perform in those patients with a Roux loop. 2005;16:615-629.
Stone fragments can be dealt with in IR by using a 7. Haskal ZJ, Martin L, Cardella JF, et al. Society of Cardio-
Dormia basket for retrieval, or can be advanced into the vascular and Interventional Radiology, Standards of
small bowel after balloon dilating the biliary tract ahead Practice Committee. Quality improvement guidelines for
of it. transjugular intrahepatic portosystemic shunts. SCVIR
Standards of Practice Committee. J Vasc Interv Radiol
2001;12:131-136.
8. Ferral H, Patel NH. Selection criteria for patients under-
Bile Leaks going transjugular intrahepatic portosystemic shunt pro-
cedures: current status. J Vasc Interv Radiol 2005;16:
Bile leaks may be seen in 10 to 15% of LT recipients. 449-455.
Many of them may be asymptomatic and detected on 9. ter Borg PC, Hollemans M, Van Buuren HR, Vleggaar FP,
protocol cholangiography as seen in minor T-tube Groeneweg M, Hop WC, Lameris JS. Transjugular intra-
leaks. These may be best followed up with repeat hepatic portosystemic shunts: long-term patency and
cholangiography to confirm closure. However, bile peri- clinical results in a patient cohort observed for 3-9 years.
Radiology 2004;231:537-545.
tonitis, sepsis, and loculated bilomas may result. PTC
10. Tripathi D, Helmy A, Macbeth K, Balata S, Lui HF, Stan-
and biliary drainage in the face of nondilated ducts is ley AJ, et al. Ten years’ follow-up of 472 patients following
possible but challenging and may provide the only non- transjugular intrahepatic portosystemic stent-shunt in-
surgical option. Noninvasive imaging with CT and US sertion at a single centre. Eur J Gastroenterol Hepatol
can easily identify biliary collections and these can be 2004;16:9-18.
percutaneously drained if needed.226 Sheng et al.227 11. Molmenti EP, Segev DL, Arepally A, Hong J, Thuluvath
PJ, Rai R, Klein AS. The utility of TIPS in the management
reported bile leaks in 4.3% of 1,363 transplants at our of Budd-Chiari syndrome. Ann Surg 2005;241:978-981;
institution. A total of 36% occurred at the biliary anas- discussion 982-983.
tomosis (95% choledochojejunostomy, 5% choledocho- 12. Rosch J, Keller FS. Transjugular intrahepatic portosys-
choledochostomy); 36% were seen at the T-tube exit temic shunt: present status, comparison with endo-
sites and 22% were seen intrahepatically, secondary to scopic therapy and shunt surgery, and future prospec-
tives. World J Surg 2001;25:337-346.
biliary necrosis.
13. Radosevich PM, Ring EJ, LaBerge JM, Peltzer MY, Haskal
Nonanastomotic leaks and leaks secondary to biliary ZJ, Doherty MM, Gordon RL. Transjugular intrahepatic
necrosis from HAT are more ominous and although PTC portosystemic shunts in patients with portal vein occlu-
may temporize these patients retransplantation is often sion. Radiology 1993;186:523-527.
needed. 14. Walser EM, NcNees SW, DeLa Pena O, Crow WN, Morgan
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
17. 346 AMESUR AND ZAJKO
RA, Soloway R, Broughan T. Portal venous thrombosis: and future possibilities. Cardiovasc Intervent Radiol
percutaneous therapy and outcome. J Vasc Interv Radiol 2002;25:251-269.
1998;9:119-127. 33. Rossle M, Siegerstetter V, Huber M, Ochs A. The first
¨
15. Wallace MJ, Madoff DC, Ahrar K, Warneke CL. Tran- decade of the transjugular intrahepatic portosystemic
sjugular intrahepatic portosystemic shunts: experience shunt (TIPS): state of the art. Liver 1998;18:73-89.
in the oncology setting. Cancer 2004;101:337-345. 34. Saxon RR, Mendel-Hartvig J, Corless CL, et al. Bile duct
16. Martin M, Zajko AB, Orons PD, et al. Transjugular intra- injury as a major cause of stenosis and occlusion in
hepatic portosystemic shunt in the management of transjugular intrahepatic portosystemic shunts: com-
variceal bleeding: indications and clinical results. Sur- parative histopathologic analysis of humans and swine. J
gery 1993;114:719-725. Vasc Interv Radiol 1996;7:487-497.
17. LaBerge JM, Ring EJ, Gordon RL, et al. Creation of tran- 35. Hausegger KA, Sternthal HM, Klein GE, Karaic R,
sjugular intrahepatic portosystemic shunts with the Stauber R, Zenker G. Transjugular intrahepatic porto-
Wallstent endoprosthesis: results in 100 patients. Radi- systemic shunt: angiographic follow-up and secondary
ology 1993;187:413-420. interventions. Radiology 1994;191:177-181.
18. Kerlan RK, LaBerge, JM, Gordon RL, Ring EJ. Transjugu- 36. Haskal ZJ, Pentecost MJ, Soulen MC, Shlansky-Gold-
lar intrahepatic portosystemic shunts: current status. berg RD, Baum RA, Cope C. Transjugular intrahepatic
Am J Roentgenol 1995;164:1059-1066. portosystemic shunt stenosis and revision: early and
19. Freedman AM, Sanyal AJ, Tisnado J, et al. Complications midterm results. Am J Roentgenol 1994;163:439-444.
of transjugular intrahepatic portosystemic shunt: a com- 37. Nazarian GK, Ferral H, Castaneda-Zuniga WR, et al. De-
prehensive review. Radiographics 1993;13:1185-1210. velopment of stenoses in transjugular intrahepatic por-
20. Silva RF, Arroyo PC Jr, Duca WJ, Silva AA, Reis LF, tosystemic shunts. Radiology 1994;192:231-234.
Cabral CM, et al. Complications following transjugular 38. Vignali C, Bargellini I, Grosso M, et al. TIPS with ex-
intrahepatic portosystemic shunt: a retrospective analy- panded polytetrafluoroethylene-covered stent: results of
sis. Transplant Proc 2004;36:926-928. an Italian multicenter study. Am J Roentgenol 2005;185:
21. Deltenre P, Mathurin P, Dharancy S, Moreau R, Bulois P, 472-480.
Henrion J, et al. Transjugular intrahepatic portosystemic 39. Ockenga J, Kroencke TJ, Schuetz T, Plauth M, Kasim E,
shunt in refractory ascites: a meta-analysis. Liver Int Petersein J, et al. Covered transjugular intrahepatic por-
2005;25:349-356. tosystemic stents maintain lower portal pressure and
22. Nazarian GK, Bjarnason H, Dietz CA, et al. Refractory as- require fewer reinterventions than uncovered stents.
cites: midterm results of treatment with a transjugular in- Scand J Gastroenterol 2004;39:994-999.
trahepatic portosystemic shunt. Radiology 1997;205:173- 40. Hausegger KA, Karnel F, Georgieva B, Tauss J, Portugal-
180. ler H, Deutschmann H, Berghold A. Transjugular intra-
23. Crenshaw WB, Gordon FD, McEniff NJ, et al. Severe hepatic portosystemic shunt creation with the Viatorr
ascites: efficacy of the transjugular intrahepatic porto- expanded polytetrafluoroethylene-covered stent-graft. J
systemic shunt in treatment. Radiology 1996;200:185- Vasc Interv Radiol 2004;15:239-248.
192. 41. Barton RE, Rosch J, Saxon RR, Lakin PC, Petersen BD,
24. Laberge JM, Somberg KA, Lake JR, et al. Two-year out- Keller FS. TIPS: short- and long-term results: a survey of
come following transjugular intrahepatic portosystemic 1750 patients. Semin Interv Radiol 1995;12:364-367.
shunt for variceal bleeding: results in 90 patients. Gas- 42. Kaufman L, Itkin M, Furth EE, Stewart C, Trerotola SO.
troenterology 1995;108:1143-1151. Detachable balloon-modified reducing stent to treat he-
25. Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, patic insufficiency after transjugular intrahepatic porto-
ter Borg PC. A model to predict poor survival in patients systemic shunt creation. J Vasc Interv Radiol 2003;14:
undergoing transjugular intrahepatic portosystemic 635-638.
shunts. Hepatology 2000;31:864-871. 43. Haskal ZJ, Middlebrook MR. Creation of a stenotic stent
26. Schepke M, Roth F, Fimmers R, et al. Comparison of MELD, to reduce flow through a transjugular intrahepatic por-
Child-Pugh, and Emory model for the prediction of survival tosystemic shunt. J Vasc Interv Radiol 1994;5:827-829.
in patients undergoing transjugular intrahepatic portosys- 44. Bolondi L, Piscaglia F, Camaggi V, Grazi GL, Cavallari A.
temic shunting. Am J Gastroenterol 2003;98:1167-1174. Review article: liver transplantation for HCC. Treatment
27. Chalasani N, Clark WS, Martin LG, et al. Determinants of options on the waiting list. Aliment Pharmacol Ther
mortality in patients with advanced cirrhosis after tran- 2003;17(Suppl 2):145-150.
sjugular intrahepatic portosystemic shunting. Gastroen- 45. Llovet JM. Updated treatment approach to hepatocellular
terology 2000;118:138-144. carcinoma. J Gastroenterol 2005;40:225-235.
28. Rajan DK, Haskal ZJ, Clark TW. Serum bilirubin and 46. Varela M, Sala M, Llovet JM, Bruix J. Treatment of hep-
early mortality after transjugular intrahepatic portosys- atocellular carcinoma: is there an optimal stratergy?
temic shunts: results of a multivariate analysis. J Vasc Cancer Treat Rev 2003;29:99-104.
Interv Radiol 2002;13:155-161. 47. Ganne-Carrie N, Trinchet JC. Systemic treatment of hep-
29. Salerno F, Merli M, Cazzaniga M, et al. MELD score is atocellular carcinoma. Eur J Gastroenterol Hepatol
better than Child-Pugh score in predicting 3-month sur- 2004;16:275-281.
vival of patients undergoing transjugular intrahepatic 48. Yao FY, Bass NM, Nikolai B, Davern TJ, Kerlan R, Wu V,
portosystemic shunt. J Hepatol 2002;36:494-500. et al. Liver transplantation for hepatocellular carcinoma:
30. Ferral H, Gamboa P, Postoak DW, et al. Survival after analysis of survival according to the intention-to-treat
elective transjugular intrahepatic portosystemic shunt principle and dropout from the waiting list. Liver Transpl
creation: prediction with model for endstage liver disease 2002;8:873-883.
score. Radiology 2004;231:231-236. 49. Yao FY, Bass NM, Nikolai B, Merriman R, Davern TJ,
31. Haskal ZJ. Interventions in portal hypertension. In: Kerlan R, et al. A follow-up analysis of the pattern and
Baum S, Pentecost MJ, eds. Abrams Angiography, Vol III. predictors of dropout from the waiting list for liver trans-
Interventional Radiology, 4th ed. Boston: Little, Brown plantation in patients with hepatocellular carcinoma: im-
and Company, 1997;525-546. plications for the current organ allocation policy. Liver
32. Bilbao JI, Quiroga J, Herrero JI, Benito A. Transjugular Transpl 2003;9:684-692.
intrahepatic portosystemic shunt (TIPS): current status 50. Mazzaferro V, Regalia E, Doci R, et al. Liver transplanta-
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
18. INTERVENTIONAL RADIOLOGY IN LT 347
tion for the treatment of small hepatocellular carcinomas special reference to living-related liver transplant donors.
in patients with cirrhosis. N Engl J Med 1996;334:693- Transpl Int 2005;18:499-505.
699. 67. Saylisoy S, Atasoy C, Ersoz S, Karayalcin K, Akyar S.
51. Yao FY, Ferrell L, Bass NM, Bacchetti P, Ascher NL, Rob- Multislice CT angiography in the evaluation of hepatic
erts JP. Liver transplantation for hepatocellular carci- vascular anatomy in potential right lobe donors. Diagn
noma: comparison of the proposed UCSF criteria with the Interv Radiol 2005;11:51-59.
Milan criteria and the Pittsburgh modified TNM criteria. 68. Wang ZJ, Yeh BM, Roberts JP, Breiman RS, Qayyum A,
Liver Transpl 2002;8:765-774. Coakley FV. Living donor candidates for right hepatic
52. Johnson EW, Holck PS, Levy AE, Yeh MM, Yeung RS. The lobe transplantation: evaluation at CT cholangiogra-
role of tumor ablation in bridging patients to liver trans- phy—initial experience. Radiology 2005;235:899-904.
plantation. Arch Surg 2004;139:825-829; discussion 69. Horton KM. CT evaluation of living related liver donors.
829-830. Crit Rev Comput Tomogr 2004;45:225-233.
53. Carr BI, ed. Hepatocellular Cancer: Diagnosis and Treat- 70. Kim JK, Kim JH, Bae SJ, Cho KS. CT angiography for
ment. Totowa, NJ: Humana Press, 2005. evaluation of living renal donors: comparison of four re-
54. Graziadei IW, Sandmueller H, Waldenberger P, Koenig- construction methods. Am J Roentgenol 2004;183:471-
srainer A, Nachbaur K, Jaschke W, et al. Chemoemboli- 477.
zation followed by liver transplantation for hepatocellular 71. Sahani D, Mehta A, Blake M, Prasad S, Harris G, Saini S.
carcinoma impedes tumor progression while on the wait- Preoperative hepatic vascular evaluation with CT and MR
ing list and leads to excellent outcome. Liver Transpl angiography: implications for surgery. Radiographics
2003;9:557-563. 2004;24:1367-1380.
55. Hayashi PH, Ludkowski M, Forman LM, Osgood M, John- 72. Sakai H, Okuda K, Yasunaga M, Kinoshita H, Aoyagi S.
son S, Kugelmas M, et al. Hepatic artery chemoemboli- Reliability of hepatic artery configuration in 3D CT an-
zation for hepatocellular carcinoma in patients listed for giography compared with conventional angiography—
liver transplantation. Am J Transplant 2004;4:782-787. special reference to living-related liver transplant donors.
56. Yao FY, Kinkhabwala M, LaBerge JM, Bass NM, Brown R Transpl Int 2005;18:499-505.
Jr, Kerlan R, et al. The impact of pre-operative loco- 73. Dodd GD III, Miller WJ, Baron RL, Skolnick ML, Camp-
regional therapy on outcome after liver transplantation bell WL. Detection of malignant tumors in end-stage cir-
for hepatocellular carcinoma. Am J Transplant 2005;5(Pt rhotic livers: efficacy of sonography as a screening tech-
1):795-804. nique. Am J Roentgenol 1992;159:727-733.
57. Roayaie S, Frischer JS, Emre SH, Fishbein TM, Sheiner 74. Crossin JD, Muradali D, Wilson SR. US of liver transplants:
PA, Sung M, et al. Long-term results with multimodal normal and abnormal. Radiographics 2003;23:1093-1114.
adjuvant therapy and liver transplantation for the treat-
ment of hepatocellular carcinomas larger than 5 centi- 75. Chong WK. Ultrasound evaluation of liver transplants.
meters. Ann Surg 2002;235:533-539. Abdom Imaging 2004;29:180-188.
58. Limanond P, Raman SS, Ghobrial RM, Busuttil RW, Saab 76. Sidhu PS, Marshall MM, Ryan SM, Ellis SM. Clinical use
S, Lu DS. Preoperative imaging in adult-to-adult living of Levovist, an ultrasound contrast agent, in the imaging
related liver transplant donors: what surgeons want to of liver transplantation: assessment of the pre- and post-
know. J Comput Assist Tomogr 2004;28:149-157. transplant patient. Eur Radiol 2000;10:1114-1126.
59. Carr JC, Nemcek AA Jr, Abecassis M, Blei A, Clarke L, 77. Sidhu PS, Shaw AS, Ellis SM, Karani JB, Ryan SM. Mi-
Pereles FS, et al. Preoperative evaluation of the entire crobubble ultrasound contrast in the assessment of he-
hepatic vasculature in living liver donors with use of patic artery patency following liver transplantation: role
contrast-enhanced MR angiography and true fast imag- in reducing frequency of hepatic artery arteriography.
ing with steady-state precession. J Vasc Interv Radiol Eur Radiol 2004;14:21-30.
2003;14:441-449. 78. Berry JD, Sidhu PS. Microbubble contrast-enhanced ul-
60. Kruskal JB, Raptopoulos V. How I do it: pre-operative CT trasound in liver transplantation. Eur Radiol 2004;
scanning for adult living right lobe liver transplantation. 14(Suppl 8):P96-P103.
Eur Radiol 2002;12:1423-1431. 79. Siegelman ES, Outwater EK. MR imaging techniques of
61. Lee VS, Morgan GR, Teperman LW, John D, Diflo T, the liver. Radiol Clin North Am 1998;36:263-284.
Pandharipande PV, et al. MR imaging as the sole preop- 80. Glockner JF, Forauer AR, Solomon H, Varma CR, Per-
erative imaging modality for right hepatectomy: a pro- man WH. Three-dimensional gadolinium-enhanced MR
spective study of living adult-to-adult liver donor candi- angiography of vascular complications after liver trans-
dates. Am J Roentgenol 2001;176:1475-1482. plantation. Am J Roentgenol 2000;174:1447-1453.
62. Sahani D, Mehta A, Blake M, Prasad S, Harris G, Saini S. 81. Stafford-Johnson DB, Hamilton BH, Dong Q, Cho KJ,
Preoperative hepatic vascular evaluation with CT and MR Turcotte JG, Fontana RJ, Prince MR. Vascular complica-
angiography: implications for surgery. Radiographics tions of liver transplantation: evaluation with gadolini-
2004;24:1367-1380. um-enhanced MR angiography. Radiology 1998; 207:153-
63. Pannu HK, Maley WR, Fishman EK. Liver transplanta- 160.
tion: preoperative CT evaluation. Radiographics 2001; 82. Hahn PF, Saini S. Liver-specific MR imaging contrast
21(Spec No):S133-S146. agents. Radiol Clin North Am 1998;36:287-297.
64. Bassignani MJ, Fulcher AS, Szucs RA, Chong WK, 83. Fulcher AS, Szucs RA, Bassignani MJ, Marcos A. Right
Prasad UR, Marcos A. Use of imaging for living donor liver lobe living donor liver transplantation: preoperative eval-
transplantation. Radiographics 2001;21:39-52. uation of the donor with MR imaging. Am J Roentgenol
65. Hollett MD, Jeffrey RB Jr, Nino-Murcia M, Jorgensen MJ, 2001;176:1483-1491.
Harris DP. Dual phase helical CT of the liver: value of 84. Bassignani MJ, Fulcher AS, Szucs RA, Chong WK,.
arterial phase scans in the detection of small ( 1.5 cm) Prasad UR, Marcos A. Use of imaging for living donor liver
malignant hepatic neoplasms. Am J Roentgenol 1995; transplantation. Radiographics 2001;21:39-52.
164:879-884. 85. Stafford-Johnson DB, Hamilton BH, Dong Q, Cho KJ, Tur-
66. Sakai H, Okuda K, Yasunaga M, Kinoshita H, Aoyagi S. cotte JG, Fontana RJ, Prince MR. Vascular complications
Reliability of hepatic artery configuration in 3D CT an- of liver transplantation: evaluation with gadolinium en-
giography compared with conventional angiography— hanced MR angiography. Radiology 1998;207:153-160.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
19. 348 AMESUR AND ZAJKO
86. Kadir S. Atlas of normal and variant angiographic anat- cular complications after liver transplantation: a 5-year
omy. Philadelphia: WB Saunders, 1991:298. experience. Am J Roentgenol 1986;147:657-663.
87. Marcucci L, Shaked A, Maller ES, et al. Supraceliac aortic 109. Quiroga S, Sebastia MC, Margarit C, Castells L, Boye R,
pseudoaneurysms after liver transplantation in infants. Alvarez-Castells A. Complications of orthotopic liver
Transplantation 1999;68:1617-1619. transplantation: spectrum of findings with helical CT.
88. Figueras J, Pares D, Aranda H, et al. Results of using the Radiographics 2001;21:1085-1102.
recipient’s splenic artery for arterial reconstruction in 110. Brancatelli G, Katyal S, Federle MP, Fontes P. Three-
liver transplantation in 23 patients. Transplantation dimensional multislice helical computed tomography
1997;64:655-658. with the volume rendering technique in the detection of
89. Nakatsuka T, Takushima A, Harihara Y, et al. Versatility vascular complications after liver transplantation.
of the inferior epigastric artery as an interpositional vas- Transplantation 2002;73:237-242.
cular graft in living-related liver transplantation. Trans- 111. Esquivel CO, Koneru B, Karrer F, et al. Liver transplan-
plantation 1999;67:1490-1492. tation before 1 year of age. J Pediatr 1987;110:545-548.
90. Todo S, Makowka L, Tzakis AG, et al. Hepatic artery in liver 112. Lallier M, Dickens SV, Dubois J, et al. Vascular compli-
transplantation. Transplant Proc 1987;19:2406-2411. cations after pediatric liver transplantation. J Pediatr
91. Starzl TE, Halgrimson CG, Koep LJ, Weil R, Taylor PD. Surg 1995;30:1122-1126.
Vascular homografts from cadaveric organ donors. Surg 113. Hesselink EJ, Klompmaker IJ, Pruim J, van Schilfgaarde
Gynecol Obstet 1979;149:737. R, Slooff MJ. Hepatic artery thrombosis after orthotopic
92. Shaw BW Jr, Iwatsuki S, Starzl TE. Alternate methods of liver transplantation: a fatal complication or an asymp-
arterialization of the hepatic graft. Surg Gynecol Obstet tomatic event. Transplant Proc 1989;21:2462.
1984;159:490-493. 114. Sarfati PO, Boillot O, Baudin F, et al. Acute hepatic
93. Tzakis A, Todo S, Stieber A, Starzl TE. Venous jump thrombosis in pediatric liver transplantation: surgical
grafts for liver transplantation in patients with portal thrombectomy and in situ fibrinolysis. Ann Chir 1992;
vein thrombosis. Transplantation 1989;48:530-531. 46:605-609.
94. Krom RAF, Kingma LM, Haagsma EB, Wesenghagen H, 115. Segel MC, Zajko AB, Bowen AD, et al. Hepatic artery
Slooff MJH, Gips CH. Choledochocholedochostomy, a thrombosis after liver transplantation: radiologic evalu-
relatively safe procedure in orthotopic liver transplanta- ation. Am J Roentgenol 1986;146:137-141.
tion. Surgery 1985;97:552-556. 116. Tzakis AG, Gordon RD, Shaw BW, Iwatsuki S, Starzl TE.
95. Friend PJ. Overview: biliary reconstruction after liver Clinical presentation of hepatic artery thrombosis after
transplantation. Liver Transpl Surg 1995;3:153-155. liver transplantation in the cyclosporine era. Transplan-
96. Van Ha TG. Liver biopsy in liver transplant recipients. tation 1985;40:667-671.
Semin Interv Radiol 2004;21:271-274. 117. Rela M, Muiesan P, Bhatnagar V, et al. Hepatic artery
97. Vautier G, Scott B, Jenkins D. Liver biopsy: blind or thrombosis after liver transplantation in children under
guided? BMJ 1994;309:1455-1456. 5 years of age. Transplantation 1996;61:1355-1357.
98. Pasha T, Gabriel S, Therneau T, Dickson ER, Lindor KD. 118. Ishigami K, Zhang Y, Rayhill S, Katz D, Stolpen A. Does
Cost-effectiveness of ultrasound guided liver biopsy. variant hepatic artery anatomy in a liver transplant re-
Hepatology 1998;27:1220-1226. cipient increase the risk of hepatic artery complications
99. Younossi ZM, Teran JC, Ganiats TG, Carey WD. Ultra- after transplantation? Am J Roentgenol 2004;183:1577-
sound- guided liver biopsy for parenchymal liver disease 1584.
an economic analysis. Dig Dis Sci 1998;43:46-50. 119. Tzakis AG. The dearterialized liver graft. Semin Liver Dis
100. Little AF, Zajko AB, Orons PD. Transjugular liver biopsy: 1985;5:375-376.
a prospective study in 43 patients with the Quick-Core 120. Langnas AN, Marujo W, Stratta RJ, et al. Hepatic allo-
biopsy needle. J Vasc Interv Radiol 1996;7:127-131. graft rescue following arterial thrombosis: role of urgent
101. Kardache M, Soyer P, Boudiaf M, Cochand-Priollet B, revascularization. Transplantation 1991;51:86-90.
Pelage JP, Rymer R. Transjugular liver biopsy with an 121. Sheiner PA, Rathna Varma CVR, Guarrera JV, et al.
automated device. Radiology 1997;204:369-372. Selective revascularization of hepatic artery thrombosis
102. Macedo G, Maia JC, Gomes A, Teixeira A, Ribeiro T. The after liver transplantation improves patient and graft
role of transjugular liver biopsy in a liver transplant cen- survival. Transplantation 1997;64:1295-1299.
ter. J Clin Gastroenterol 1999;29:155-157. 122. Northover JMA, Terblanche J. A new look at the arterial
103. Bruzzi JF, O’Connell MJ, Thakore H, O’Keane C, Crowe supply of the bile duct in man and its surgical implica-
J, Murray JG. Transjugular liver biopsy: assessment of tions. Br J Surg 1979;66:379-384.
safety and efficacy of the Quick-Core biopsy needle. Ab- 123. Northover J, Terblanche J. Bile duct blood supply: its
dom Imaging 2002;27:711-715. importance in human liver transplantation. Transplan-
104. Blumhardt G, Ringe B, Lauchart W, Burdelski M, Bech- tation 1978;26:67-69.
stein WO, Pichlmayr R. Vascular problems in liver trans- 124. Orons PD, Sheng R, Zajko AB. Hepatic artery stenosis in
plantation. Transplant Proc 1987;9:2412. liver transplant recipients: prevalence and cholangio-
105. Langnas AN, Marujo W, Stratta RJ, Wood RP, Shaw BW graphic appearance of associated biliary complications.
Jr. Vascular complications after orthotopic liver trans- Am J Roentgenol 1995;165:1145-1149.
plantation. Am J Surg 1991;161:76-83. 125. Zajko AB, Campbell WL, Logsdon GA, et al. Cholangio-
106. Letourneau JG, Castaneda-Zuniga WR. The role of radi- graphic findings in hepatic artery occlusion after liver
ology in the diagnosis and treatment of biliary complica- transplantation. Am J Roentgenol 1987;149:485-489.
tions after liver transplantation. Cardiovasc Intervent 126. De Candia A, Como G, Tedeschi L, et al. Color Doppler
Radiol 1990;13:278-282. sonography of hepatic artery reconstruction in liver
107. Marujo WC, Langnas AN, Wood RP, Stratta RJ, Li S, transplantation. J Clin Ultrasound 2002;30:12-17.
Shaw BW Jr. Vascular complications following ortho- 127. Garcia-Criado A, Gilabert R, Nicolau C, Real I, Arguis P,
topic liver transplantation: outcome and the role of ur- Bianchi L, et al. Early detection of hepatic artery throm-
gent revascularization. Transplant Proc 1991;23:1484- bosis after liver transplantation by Doppler ultrasonog-
1486. raphy: prognostic implications. J Ultrasound Med 2001;
108. Wozney P, Zajko AB, Bron KB, Point S, Starzl TE. Vas- 20:51-58.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
20. INTERVENTIONAL RADIOLOGY IN LT 349
128. Cook GJR, Crofton ME. Hepatic artery thrombosis and 145. Gazzera C, Doriguzzi Breatta A, Veltri A, Righi D, Barbero
infarction: evolution of the ultrasound appearances in S, Balderi A, et al. Femoral haemostosis with vasoseal
liver transplant recipients. Br J Radiol 1997;70:248-251. ES: experience in 150 patients. Radiol Med (Torino)
129. Nghiem HV, Tran K, Winter TC, et al. Imaging of compli- 2005;109:118-124.
cations in liver transplantation. Radiographics 1996;16: 146. Hirsch JA, Reddy SA, Capasso WE, Linfante I. Non-inva-
825-840. sive hemostatic closure devices: “patches and pads”.
130. Flint EW, Sumkin JH, Zajko AB, Bowen A. Duplex sonog- Tech Vasc Interv Radiol 2003;6:92-95.
raphy of hepatic artery thrombosis after liver transplan- 147. Koreny M, Riedmuller E, Nikfardjam M, Siostrzonek P,
tation. Am J Roentgenol 1988;151:481-483. Mullner M. Arterial puncture closing devices compared
131. Dodd GD, Memel DS, Zajko AB, Baron RL, Santaguida with standard manual compression after cardiac cathe-
LA. Hepatic artery stenosis and thrombosis in transplant terization: systematic review and meta-analysis. JAMA
recipients: Doppler diagnosis with resistive index and 2004;291:350-357.
systolic acceleration time. Radiology 1994;192:657-661. 148. Sheiner PA, Varma CV, Guarrera JV, Cooper J, Garatti M,
132. Kaneko J, Sugawara Y, Akamatsu N, Kishi Y, Kokudo N, Emre S, et al. Selective revascularization of hepatic artery
Makuuchi M. Implantable Doppler probe for continuous thromboses after liver transplantation improves patient
monitoring of blood flow after liver transplantation. and graft survival. Transplantation 1997;64:1295-1299.
Hepatogastroenterology 2005;52:194-196. 149. Abad J, Hidalgo EG, Cantarero JM, et al. Hepatic artery
133. Boyvat F, Aytekin C, Firat A, Harman A, Karakayali H, anastomotic stenosis after transplantation: treatment
Haberal M. Diagnostic and therapeutic management of with percutaneous transluminal angioplasty. Radiology
hepatic artery thrombosis and stenosis after orthotopic 1989;171:661-662.
and heterotopic liver transplantation. Transplant Proc 150. Castaneda F, So SK, Hunter DW, Castaneda-Zuniga WR,
2003;35:2791-2795. Amplatz K. Reversible hepatic transplant ischemia: case
134. Hidalgo EG, Abad J, Cantarero JM, et al. High dose report and review of literature. Cardiovasc Intervent Ra-
intraarterial urokinase for the treatment of hepatic ar- diol 1990;13:88-90.
tery thrombosis in liver transplantation. Hepatogastro- 151. Orons PD, Blessios GA, Zajko AB, Sammon JK, Mazer-
enterology 1989;36:529-532. iegos G. Hepatic artery angioplasty after liver transplan-
135. Figueras J, Busquets J, Dominguez J, et al. Intra-arterial tation: long-term results in 42 patients. 83rd Scientific
thrombolysis in the treatment of acute hepatic artery Assembly and Annual Meeting of the Radiological Society
thrombosis after liver transplantation. Transplantation of North America, Chicago, IL, November 30-December 5,
1995;59:1356-1357. 1997.
136. Loupatatzis C, Stoupis C, Seiler C, Candinas D, Do DD, 152. Orons PD, Zajko AB, Bron KM, Trecha GT, Selby RR,
Triller J. Use of a mechanical thrombectomy device to Fung JJ. Hepatic artery angioplasty after liver transplan-
recanalize a subacutely occluded aortohepatic bypass tation: experience in 21 allografts. J Vasc Interv Radiol
after orthotopic liver transplantation. J Endovasc Ther 1995;6:523-529.
2005;12:401-404. 153. Propst A, Waldenberger P, Propst T, Vogel W, Konig-
137. Yilmaz S, Kirimlioglu V, Isik B, Yilmaz M, Kirimlioglu HS, srainer A, Jaschke W. Spasms of the hepatic artery fol-
Ara C, et al. Urgent revascularization of a liver allograft lowing percutaneous transluminal angioplasty and tola-
with a saphenous vein interposition graft between the zoline administration in a liver transplant patient.
hepatic artery and the recipient splenic artery after late Cardiovasc Intervent Radiol 1996;19:181-183.
hepatic artery thrombosis. Dig Dis Sci 2005;50:1177- 154. Narumi S, Osorio RW, Freise CE, Stock PG, Roberts JP,
1180. Ascher NL. Hepatic artery pseudoaneurysm with hemo-
138. Vignali C, Bargellini I, Cioni R, Petruzzi P, Cicorelli A, bilia following angioplasty after liver transplantation.
Lazzereschi M, et al. Diagnosis and treatment of hepatic Clin Transplant 1998;12:508-510.
artery stenosis after orthotopic liver transplantation. 155. Sheng R, Orons PD, Ramos H, Zajko AB. Dissecting
Transplant Proc 2004;36:2771-2773. pseudoaneurysm of the hepatic artery: a delayed compli-
139. Bechstein WO, Blumhardt G, Ringe B, et al. Surgical cation of angioplasty in a liver transplant. Cardiovasc
complications in 200 consecutive liver transplants. Intervent Radiol 1995;18:112-114.
Transplant Proc 1987;19:3830-3831. 156. Bechstein WO, Blumhardt G, Ringe B, et al. Surgical
140. Raby N, Karani J, Thomas S, O’Grady J, Williams R. complications in 200 consecutive liver transplants.
Stenoses of vascular anastomoses after hepatic trans- Transplant Proc 1987;19:3830-3831.
plantation: Treatment with balloon angioplasty. Am J 157. Fichelle JM, Colacchio G, Castaing D, Bismuth H. In-
Roentgenol 1991;157:167-171. fected false hepatic artery aneurysm after orthotopic liver
141. Toursarkissian B, Mejia A, Smilanich RP, Shireman PK, transplantation treated by resection and reno-hepatic
Sykes MT. Changing patterns of access site complica- vein graft. Ann Vasc Surg 1997;11:300-303.
tions with the use of percutaneous closure devices. Vasc 158. L’Hermine C, Ernst O, Delemazure O, Sergent G. Arterial
Surg 2001;35:203-206. complications of transhepatic biliary drainage. Cardio-
142. Gonze MD, Sternbergh WC 3rd, Salartash K, Money SR. vasc Intervent Radiol 1996;19:160-164.
Complications associated with percutaneous closure de- 159. Karatzas T, Lykaki-Karatzas E, Webb M, et al. Vascular
vices. Am J Surg 1999;178:209-211. complications, treatment, and outcome following ortho-
143. Sanborn TA, Gibbs HH, Brinker JA, Knopf WD, Kosinksi topic liver transplantation. Transplant Proc 1997;29:2853-
EJ, Roubin GS. A multicenter randomized trial compar- 2855.
ing a percutaneous collagen hemostasis device with con- 160. Kim HJ, Kim KW, Kim AY, Kim TK, Byun JH, Won HJ, et al.
ventional manual compression after diagnostic angiog- Hepatic artery pseudoaneurysms in adult living-donor liver
raphy and angioplasty. J Invasive Cardiol 1999;11(Suppl transplantation: efficacy of CT and Doppler sonography.
B):6B-13B. Am J Roentgenol 2005;184:1549-1555.
144. Hong K, Liapi E, Georgiades CS, Geschwind JF. Case- 161. Madariaga J, Tzakis A, Zajko AB, et al. Hepatic artery
controlled comparison of a percutaneous collagen arte- pseudoaneurysm ligation after orthotopic liver trans-
riotomy closure device versus manual compression after plantation: a report of 7 cases. Transplantation 1992;54:
liver chemoembolization. J Vasc Interv Radiol 2005;16: 824-828.
339-345. 162. Bonham CA, Kapur S, Geller D, Fung JJ, Pinna A. Exci-
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases