Download as PDF, PPTX





















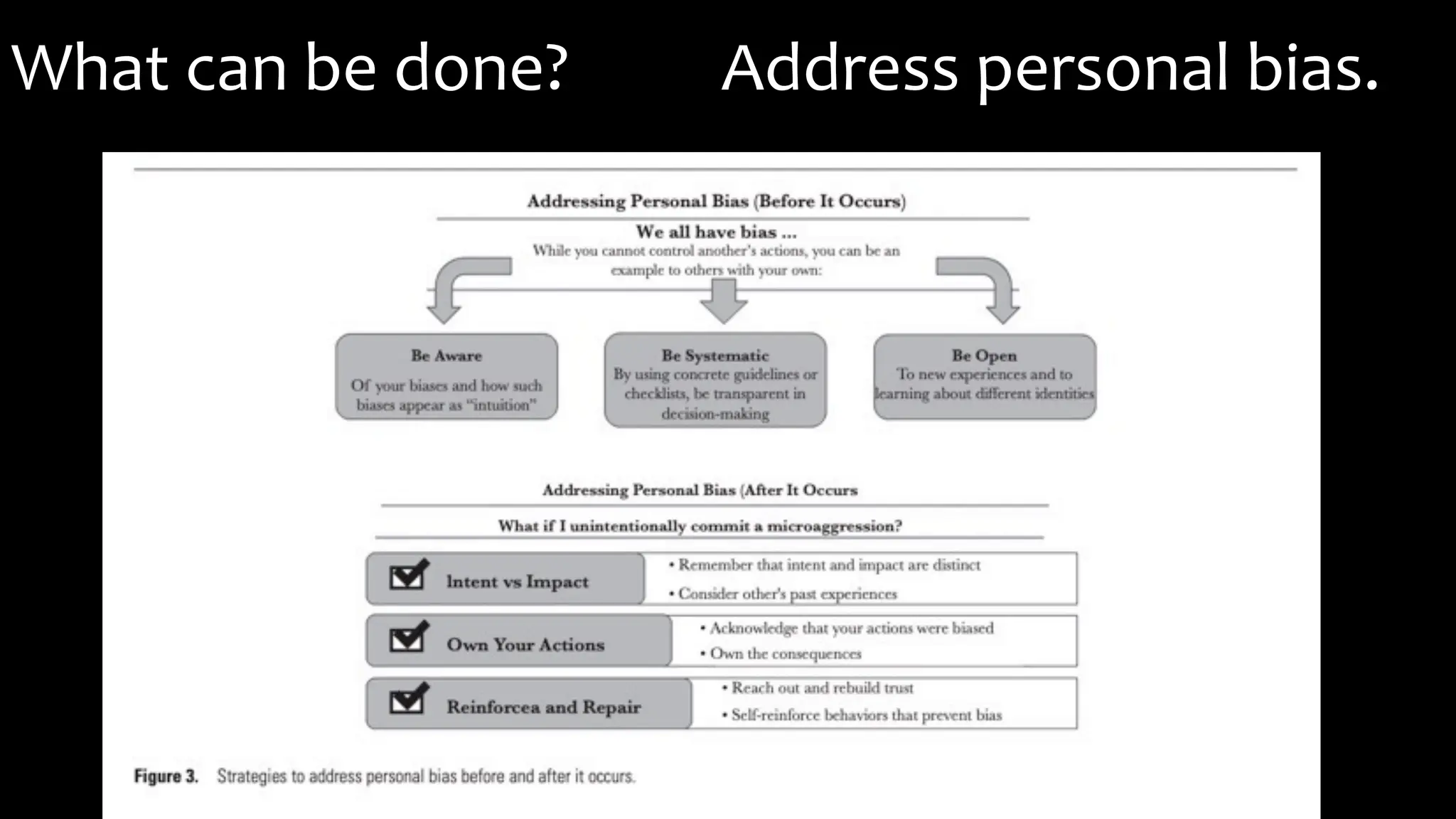













The document provides an evidence-based overview of bias in healthcare, detailing various types of bias, including weight, racial, gender, and class biases, and their detrimental effects on patient care and health outcomes. It explores the concepts of systemic racism, health disparities, and health inequities, emphasizing the role of cultural trauma and epigenetics in perpetuating these issues within marginalized communities. The presentation also discusses ways to combat bias through personal accountability, training, and policy changes in the healthcare system.























































































