Downloaded 75 times


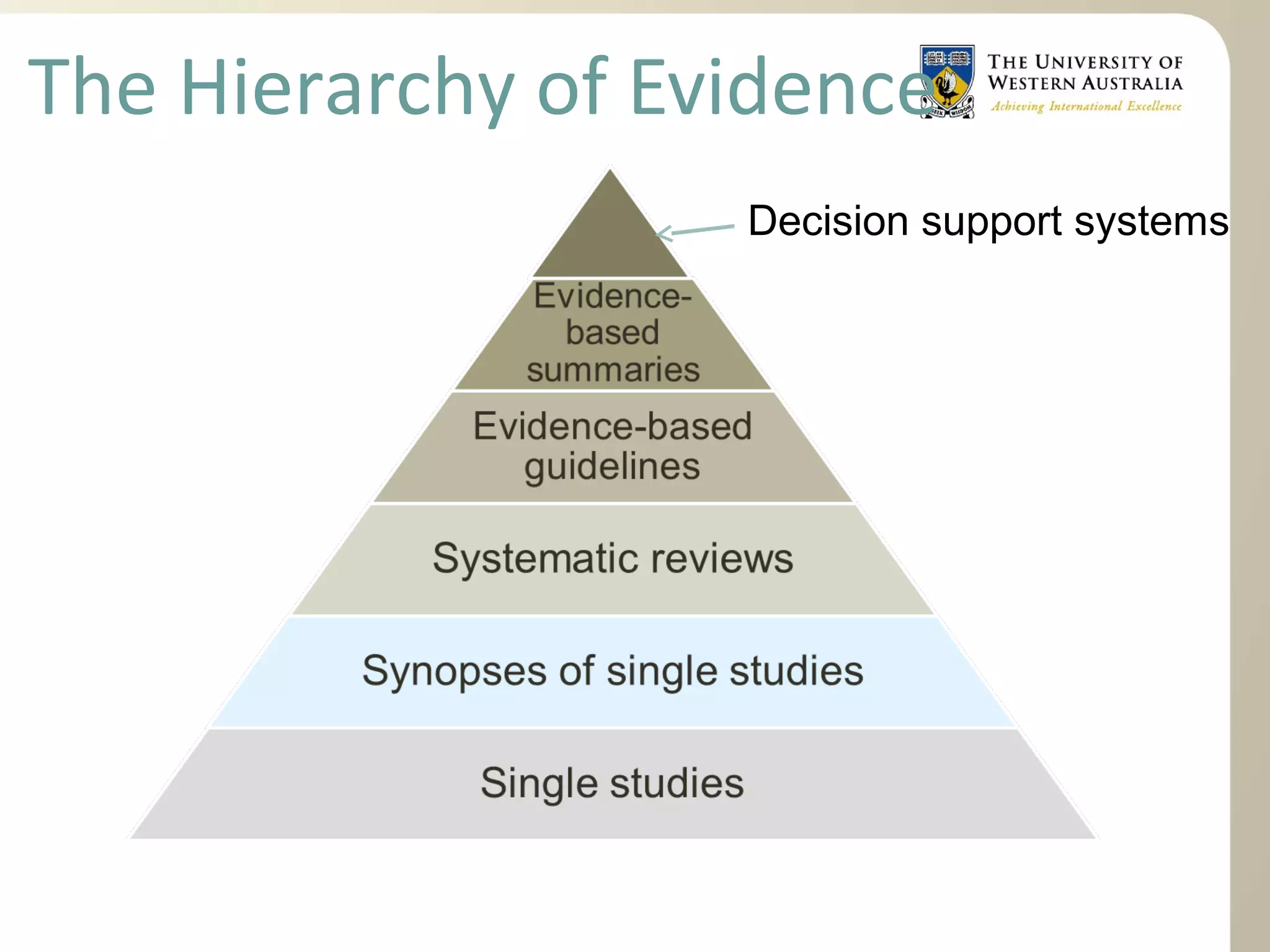

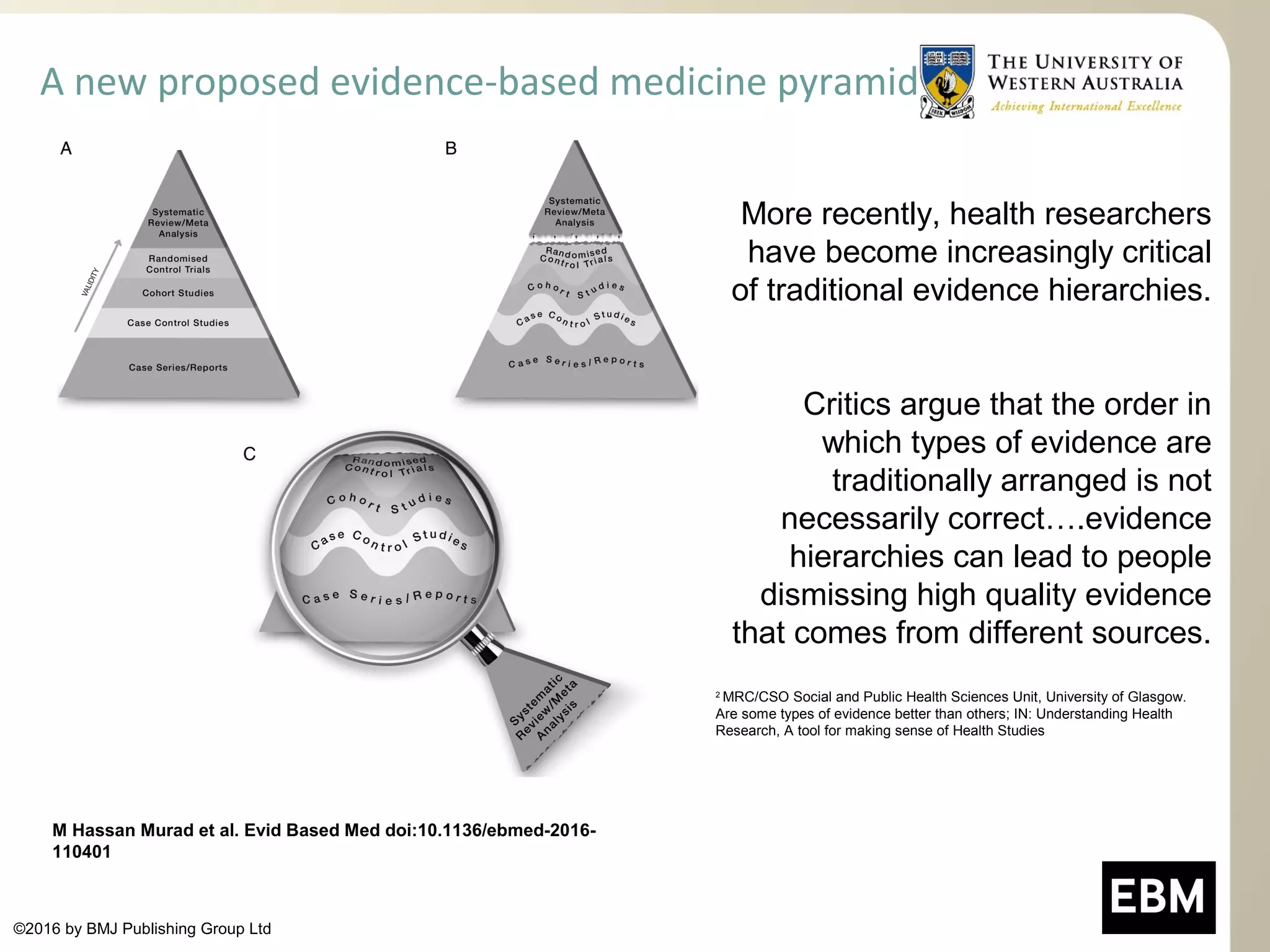








The document outlines the concept of hierarchies of evidence in health research, highlighting traditional levels of evidence and the shift towards systematic reviews as preferred methods for summarizing research. It discusses critiques of existing evidence hierarchies and emphasizes the importance of various evidence sources in decision-making. Additionally, it provides resources for locating evidence and contrasts databases like Medline and PubMed.























































































