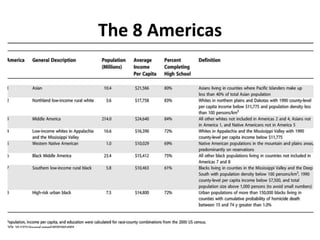
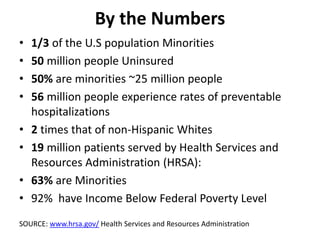
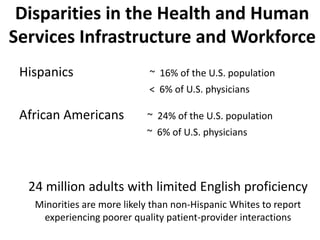
Health care disparities exist between different racial and ethnic groups in the United States. The WHO defines health disparities as differences in health outcomes that are closely linked to social and economic disadvantage. There can be up to a 33 year difference in life expectancy between racial groups. Disparities are driven by social determinants like education, income, and environment. Minority groups face greater barriers to accessing quality health care due to lack of insurance, language barriers, and provider biases. Addressing disparities requires improvements in data collection, the health workforce, and policies aimed at promoting equity.